
Missionaries spread disinfo and fear about vaccine to indigenous communities
By Nathalia Urban
Indigenous communities are considered a priority group in vaccination against COVID-19 in Brazil, but due to the influence of missionaries some public health agents are facing hostility and even threats from some communities.
In the race to guarantee the immunization of indigenous peoples, a logistics that implies difficulties such as facing long distances and difficulties in accessing villages, especially when talking about the Amazon, the challenge now arises to convince them that the vaccine is safe and it is the only guarantee against the new coronavirus. In the Brazilian Amazon alone, there are 32,927 confirmed cases and 760 deaths due to Covid-19, according to a newsletter updated until February 1 by the Coordination of Indigenous Organizations in the Amazon (Coiab). Across the country, Covid-19 killed 948 indigenous people until February 4th, according to the Articulation of Indigenous Peoples of Brazil (Apib). Around 47,752 cases of Covid-19 have been confirmed in 161 different indigenous people.
The Jamamadi people say they will only accept health teams into the village if Stuart Campbell a North-American missionary, from the Greene Baptist Church participated.
The local authorities negotiated with the missionary and promised the indigenous people that he would accompany the vaccinations, but, after last-minute clashes, his presence on the team was canceled. The Jamamadi revolted and the situation worsened.
Problems between local authorities and indigenous communities caused by Campbell are not news. In 2018, the missionary was expelled from the region by authorities after having illegally entered the land of the isolated Indians of the Hi-Merimã ethnicity, which is close to the Jamamadi.
By preventing Indigenous Health District officials from entering the villages, the health of the Jamamadi is helpless. With a population of 399 people, according to a census by the Special Secretariat for Indigenous Health (Sesai) in 2020, some people use leprosy, hypertension and other medications. But they are without treatment, according to the report, as some indigenous people, led by their leader Cacique Abadias Jamamadi, do not authorize the delivery of the medication.
The restoration of healthcare is conditional on the missionary’s return to the region, as shown in a document obtained by the Bocado report. “We have been in trouble since 2019, but it intensified in 2020, when service in the village was interrupted”, reports an employee who works in the region. “There are threats to the professionals who work there and the missionary interferes in all dialogue with the Jamamadi.”
Other communities are facing the same ongoing issues like the ones located near the municipality of Santo Antônio do Içá, in the Amazon, were the indigenous people are also refusing to receive the vaccine against Covid-19 because of the influence of evangelical pastors.
Perpétua Tsuni, leader of the Kokama people from that region, told UOL that religious leaders spread lies among members of local communities, that “the vaccine would transform them in animals, homosexuals, or even kill them. They’ve also mentioned that the vaccine microchip would carry the ‘mark of the beast’”.
The vaccine is not mandatory in the country, so statements of responsibility are being prepared by health professionals working in the region so that indigenous people who refuse to receive the dose can sign, thus making them responsible for possible consequences of contamination by the coronavirus.
In Brazil, indigenous communities have the right to remain isolated. It is a law instituted in 1987, in the midst of the drafting of the new Constitution, which recognized a series of other rights which were previously denied.
The presence of evangelical missionaries and pastors in indigenous lands, often seeking to change the worldviews of indigenous peoples, has been discussed for many years. Due to the alarming refusal of the vaccine, on the 26 of January, APIB launched a collective action to guarantee vaccination in Brazilian indigenous lands with the hashtag #VacinaParente.
On its social media and in contact with grassroots organizations, the entity has passed on the videos produced autonomously by local leaders, which aim to encourage the population to adhere to the vaccination programme. The campaign is a response to the anti-vaccine crusade that has led many indigenous people to avoid immunization.
https://www.brasilwire.com/missionaries ... mmunities/
God damn the missionaries.
Socialist Demands for the COVID-19 Crisis
Re: Socialist Demands for the COVID-19 Crisis
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis

Jeff Bezos, recently retired CEO of Amazon, whose warehouses were notoriously unhygienic
What coronavirus taught us about the ruling class
Posted Feb 23, 2021 by Ben Hillier
Originally published: Red Flag (February 20, 2021) |
If half a million people in the United States were murdered by an evil cult, the leaders of which said that they would keep killing thousands a day to satisfy their rapacious urge for power and money, what do you think the response would be?
The last U.S. mass casualty event that came close in scale was the 2001 terrorist attacks, when some 3,000 people were killed in a single day. The reaction after 9/11 was swift and dramatic. All levels of government decried the loss of innocent life. The White House launched a “war on terror”, spending $6.4 trillion by 2019, according to the Watson Institute of International and Public Affairs, and established an entirely new federal government department, Homeland Security, which is the third largest.
Congress passed the Patriot Act, which was used to justify a mass surveillance program over the entire population to find anyone remotely sympathetic to the murderers. The corporate media relentlessly denounced the evil masterminds of the attacks and the detestable, radical ideology that motivated them. A special facility at Guantánamo Bay was established to jail and torture anyone perceived to be involved. Muslims were rounded up in the U.S. and around the world. Hundreds of thousands were killed in Iraq and Afghanistan as more than 1.5 million troops were rotated through those countries over the next two decades.
It was as close as a country gets to a “total mobilisation”—mustering public sentiment, almost all media outlets, the entire political class and education system, from primary schools to universities, and recruiting and directing a huge array of national resources and human activity to a single end. All of it, allegedly, was for the safety and wellbeing of U.S. citizens: to make sure that the World Trade Center deaths would not be in vain and to prevent such a loss of life ever happening again.
We know that there was a great deal of bullshit and lies in the response, that the terrorist attacks were used as a pretext for wars that sections of the political and military establishment were intent on waging anyway. But still, you might think that, if there were a series of mass casualty events claiming the lives of 3,000 people per day over an extended period, reaching a total of half a million deaths, with no end in sight, every level of government in the United States might mobilise resources in an unprecedented way to stop the carnage, right?
Yet what we in fact see are state and federal governments, Republican and Democratic alike, overseeing the deaths, which are indeed close to 500,000 in just one year. The U.S. ruling class has allowed the coronavirus to become endemic in the population because of a twisted ideology that valorises corporate profits above human life.
It’s not just the United States. Around the world, the response has been similar. Britain lost 70,000 civilian lives in all of World War Two. Nearly 120,000 have perished in just one year of this pandemic. France has lost more than 80,000, Italy more than 90,000, Spain and Germany more than 60,000 each. Brazil is close to one-quarter of a million. Mexico 170,000. India more than 150,000. The global total is close to 2.4 million.
And nowhere has the response come anywhere close to the frenzy after 9/11. The nature of the government has made little difference. Far-right, centre-right, liberal and centre-left administrations have all shown that their loyalties are one and the same. When the conflict emerges between making profits and saving human life, invariably the latter has been sacrificed.
There have been half measures here and there, and belated lockdowns or mask mandates in several countries when the hospitalisation and death rates got so high that the capitalist economy was being battered anyway. But at each opportunity, any serious attempt to bring community transmission under control was abandoned to allow businesses to resume making profits.
The approach is akin to waiting days after a major accident to admit a car crash victim to hospital, in the hope of saving money, then sending them home with only half their still bleeding wounds sutured and dressed, again to save on expenses.
Yet the countries with the worst outcomes have generally been the ones with the most resources and wealth. The enormous resources at their disposal—resources that are outlaid in the blink of an eye to launch a war, to give as handouts to the rich, to fund corporate welfare and company tax cuts—have simply not been deployed on a scale that would come close to addressing the challenge.
It’s not a case of unfortunate errors and miscalculations. They simply do not care. In almost every country, they have attacked as enemies of freedom those advocating measures to bring the death rate down decisively. They have again and again tried to downplay the seriousness of the situation and accused their opponents of overreacting.
Why? Because unlike an event like 9/11 in the United States, or some of the other terrorist attacks in Europe that in some instances have claimed only one or two lives, all obvious responses to the pandemic involve significant and ongoing spending on the health and welfare of workers and the poor—when the rich and powerful have spent decades cutting spending in those areas. If they were to engage in mass public spending to protect the lives and livelihoods of the majority of the population, it would only raise the question: Why can’t this be “the norm”, instead of the trillions spent on war and big business tax cuts?
Try as they might, it is difficult for politicians and their corporate media and big-business backers to leverage the pandemic for nefarious ends like war, corporate tax cuts or attacks on social spending in the name of national unity. They cannot credibly blame China (not that it stops them) or “radical Islam” for the overflowing hospitals. It’s down to them, and they know it.
Almost the entire world over, the ruling class response is to hope that the vaccines, from which their friends in the pharmaceutical industry will make billions of dollars, will put an end to the worst of it. Yet the rich countries have bought up the lion’s share, meaning that the virus will continue to devastate poor countries.
In the meantime, as mutant coronavirus strains spread across the planet, bringing into question the efficacy of the new vaccines, it’s business as usual: thousands dying every day because there’s still money to be made. It tells you everything you need to know about how the ruling class thinks—and what they think the rest of us are really worth.
https://mronline.org/2021/02/23/what-co ... ing-class/
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis
BIG PHARMA: BULLYING AND APARTHEID WITH COVID VACCINES
Eder Peña
4 Mar 2021 , 11:39 am .

Big Pharma, spoiled companies of capitalism (Photo: The Motley Food)
By mid-February, the global pandemic had infected at least 109 million people worldwide and caused more than 2.4 million deaths after a year. Its effects have cost 28 trillion dollars in production losses worldwide, and developed countries would have contracted economically by 7% in 2020.
One of the critical issues that has not made it possible to overcome the pandemic, in addition to the contradictions evidenced (one by one) of global capitalism, has to do with the slowness in the development and distribution of preventive covid-19 vaccines.
When talking about "slowness", one might think that it is only a question of criticizing the time it took for pharmaceutical companies to develop and test vaccine candidates, but the issue goes deeper: Since the SARS outbreak in 2002, another coronavirus, several Scientific sectors repeatedly warned about the risk of a pandemic but the big pharmaceutical companies (Big Pharma) refused to do any research on it because there were no expectations of profits at the time.
Even in 2016 the World Health Organization (WHO) placed coronaviruses among the eight main viral threats that required more investigation, the result is known: Last year we were not prepared for the arrival of SARS-CoV-2.
This and other avoidable delays in preventive vaccination (as the most effective measure) are imposing burdens on the global economy and human well-being in a context where economic upheavals demand more relief and recovery measures as powers play at self-preservation.
BIG PHARMA, SPOILED BY CAPITALISM
The capital of the pharmaceutical industry is concentrated in ten companies, this is greater in the production of vaccines because almost all the knowledge is in the hands of GSK, Johnson & Johnson, Pfizer and Sanofi.
Almost all Research and Development (R&D) is done in government and university laboratories paid for by taxpayers, and the sector also has tax credits and other financial concessions to cover possible risks. As drugs are developed, these companies can patent them and both consumers and governments are then charged high prices.
Their profit margins are appreciably higher across all industries, speaking of a yield of 17.3 percent compared to an average of 11.5 percent in the rest. They tend to "forget" to pay taxes on their soaring earnings to the point that only the first four big pharma evade $ 3.8 billion in taxes a year, according to the NGO Oxfam .
It would be possible to defend them if those super earnings were used for innovation and investments but they spend more on paying dividends and buying back their own shares than on R&D. Also, almost a fifth of all profits go to marketing and advertising .

Most Big Pharma invests more in sales and marketing than in research and development because the latter is done by governments (Photo: Statista)
Finally, of all the research and development in Europe, only one tenth is truly innovative. The other 90% are so-called "imitation drugs" (in English "me-too drugs") or drugs that make small changes to an existing drug.
By the end of 2020, Pfizer had sold more than 80% of the vaccine doses it could produce by the end of 2021 to governments representing 14% of the world's population. In other words, if this had been the first safe and effective vaccine to hit the market, the vast majority of the world's population would have had almost no access to it.
PFIZER AND ITS HIGH-LEVEL BULLYING
The big pharma Pfizer has entered, again, the media controversy because The Bureau of Investigative Journalism (TBIJ) published a report in which it is accused of bullying (intimidation) to, at least, three Latin American governments in the Covid vaccine negotiations and has asked some countries, such as Argentina and Brazil, to put up sovereign assets, such as embassy buildings and military bases, as collateral against the cost of any future legal cases.
In neither case was a national agreement reached, even though such delays in receiving vaccines by countries mean more infections and, consequently, more deaths.
In the case of another country, whose name is hidden by the authors of the report, the demands of the big pharma caused a delay of three months in the agreement on vaccines. Pfizer has held talks with more than 100 countries and supranational organizations, in Latin America and the Caribbean it has reached agreements, the terms of which are unknown, with Chile, Colombia, Costa Rica, the Dominican Republic, Ecuador, Mexico, Panama, Peru and Uruguay.
Pfizer negotiators demanded that recipient countries pay the potential costs of civil lawsuits that arise as a result of the company's own acts of negligence, fraud or malice if the vaccines caused injury, disability or death after being inoculated. This was described as "high-level intimidation" by an official who was present at the negotiations in the unidentified country.
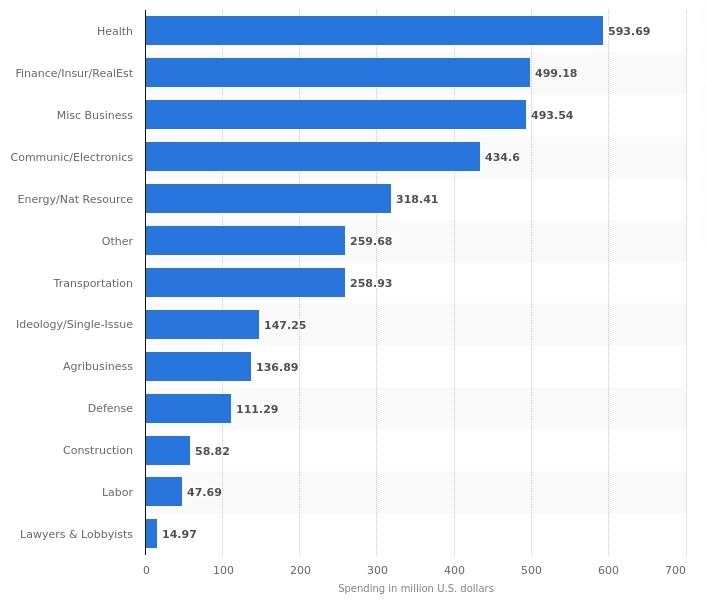
Spending on lobbies (pressure) in the United States reached almost 3.5 billion dollars in 2019, the highest in 9 years, Big Pharma (health) were the ones that spent the most (Photo: Statista)
For its part, Pfizer told TBIJ that "Globally, we have also allocated doses to low- and lower-middle-income countries at a non-profit price, including an advance purchase agreement with Covax to provide up to 40 million doses in 2021. We are committed to supporting efforts to provide developing countries with the same access to vaccines as the rest of the world, "declining to comment on the ongoing private negotiations.
As the manufacturers have developed vaccines quickly and because they protect all members of society, governments usually agree to cover the cost of compensation and, thus, if a citizen who suffers an adverse effect after being vaccinated can present a claim against the manufacturer and, if successful, the government would pay the compensation.
This places an additional burden on some countries, as it means having to hire specialized lawyers and, at times, pass complex new legislation, in order to exempt manufacturers from their responsibilities.
In the case of Argentina, an official told TBIJ that Congress approved a new law in October that allowed it, but that was not enough for Pfizer, it was not happy with the drafting of the legislation because the government believed that they should take responsibility for it. any act of negligence or malice.
The government offered to amend the existing law to make it clear that "negligence" meant problems in the distribution and delivery of vaccines (inadvertent interruption of the vaccine's cold chain, for example), but Pfizer remained dissatisfied. He asked the government to modify the legislation through a new decree and President Alberto Fernández refused.
In late December, Pfizer asked the government to put up sovereign assets such as federal bank reserves, embassy buildings or military bases as collateral. One of the reasons the government wanted Pfizer's vaccines was because the company said they could be delivered quickly. However, in the contract, Pfizer wanted to reserve the right to change the schedule. There was no room for negotiation.
APARTHEID AND THE GLOBAL FUNNEL LAW
In a world in which elites privilege the disappearance or minimization of states, the pharmaceutical business consists of financing governments to research and develop vaccines and shifting the possible costs of adverse effects onto ... governments , this includes low- and middle-income countries.
This is how BioNTech, a partner of Pfizer, received 445 million dollars from the German government to develop a vaccine, and the US government agreed last July to an agreement to pre-order 100 million doses for almost 2 billion dollars, before the vaccine would have even entered phase three of the trials. Pfizer expects to sell $ 15 billion worth of vaccines in 2021, 7.5 times more.
But the development of the vaccine is one thing, its production and distribution is another. Marc Vandepitte says that vaccine manufacturers have little interest in rapidly and massively increasing their own production capacity. Increasing the production capacity in six months would leave the new infrastructure empty instantly because the profitable business consists of the current: That the existing factories produce for years at their current capacity.
By the end of 2021, the total global capacity of the top 13 COVID-19 vaccine manufacturers would still be well below the needs of the world's nearly 7.7 billion people. Even if everyone produces to the maximum of their capacity, a fifth of the world's population would not have access until 2022.
There is a kind of apartheid to more than 85 poor countries that will not have public access to vaccines before 2023 due to patent protections, limitations on vaccine production and the accumulation of rich countries. Until last February 5, not a single dose had been administered in 130 countries with 2.5 billion people.
Of the more than 131 million doses available as of February 8, the United States, China, the European Union and the United Kingdom had 78% while Africa had 0.2%. The African Union (AU) has only asked for 670 million doses, less than half of what it needs to achieve herd immunity. In addition to Brazil, other Latin American countries only have 150 million doses for less than a quarter of their population.
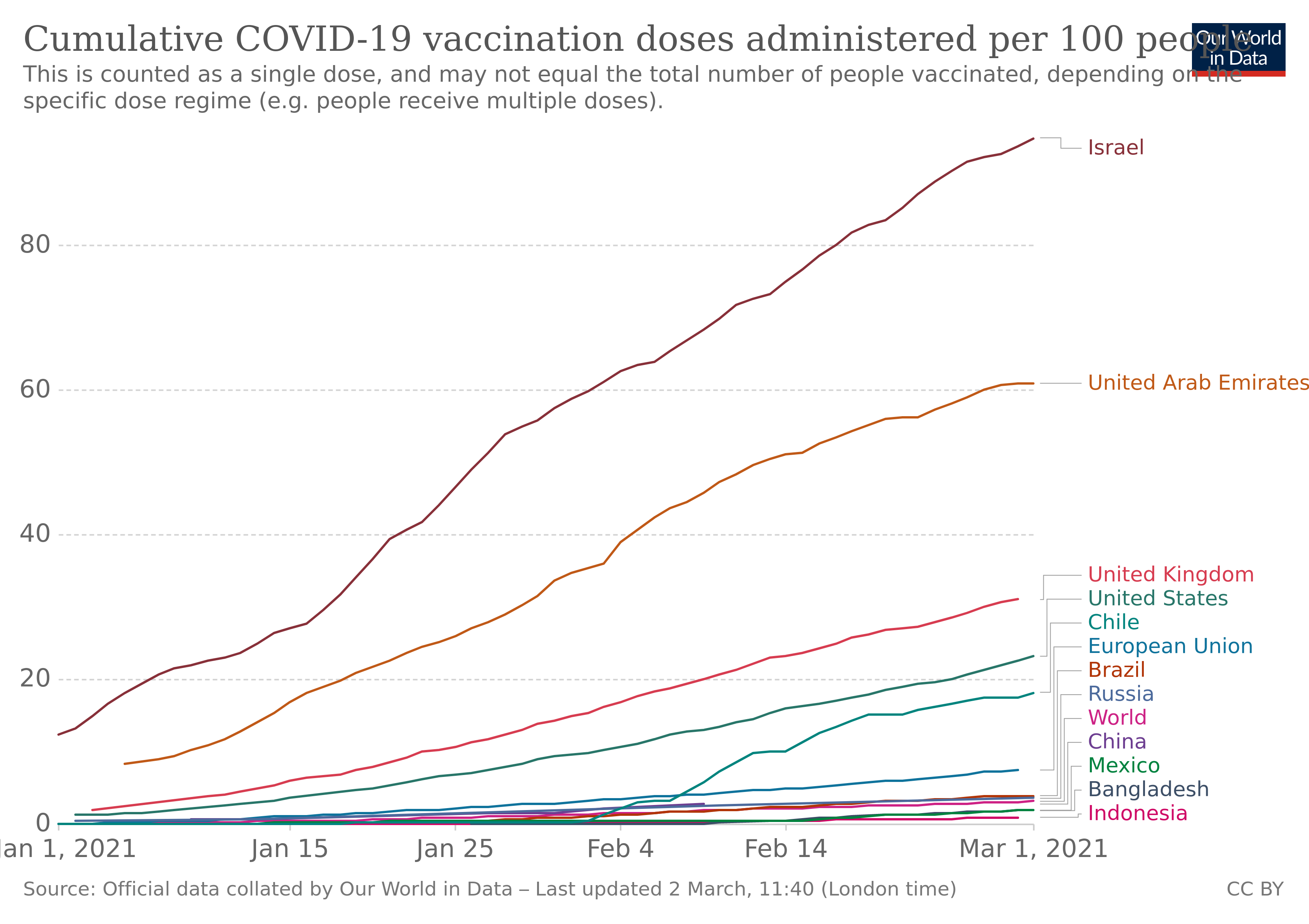
Doses of anticovid vaccines administered per 100 people in various countries since last January (Photo: Our world in data)
Global needs far exceed available supply, and middle-income countries have joined the struggle by making direct and non-transparent deals with vaccine suppliers, usually in worse conditions than if they had bargained collectively. Divided and naturally out-of-date, it's no wonder that vaccine prices vary considerably, by more than 12 times, from $ 6 to $ 74 per dose.
This so-called "vaccine imperialism" contrasts with the "vaccine nationalism" that the great powers apply to themselves, this chapter the law of the global funnel deals with how, after its dispute with AstraZeneca , the European Commission (EC) banned the vaccine exports to most countries outside the EU.
Even though the AstraZeneca vaccine was "tested" in the South African population, this country is paying 2.4 times more than the EU: $ 5.25 versus $ 2.16. Gone was the promise of "benefit sharing" and "priority access after the trial", much further for Uganda, which is paying 20% more than South Africa.
VACCINES FOR EVERYONE?
The Global Covid-19 Vaccine Access Mechanism (COVAX) is led by WHO, the Coalition for Innovations in Epidemic Preparedness and the Alliance for Vaccines (Gavi) and aims to accelerate vaccine development, ensure doses for all countries and distribute it fairly, starting with the highest risk groups.
Although it was created, in part, to prevent hoarding by the governments of rich countries, and so far more than 180 countries, representing almost two-thirds of the world's population, have joined, the results are obvious.
Among the 180 countries are 94 high-income countries that have made legally binding commitments. Everyone will have access to the vaccines on the COVAX list, and will pay for their doses individually. The 92 lower-income countries that are part of the device will receive their doses for free.
The COVAX plan consists of two phases:
Phase 1: All participating countries would receive doses proportional to their populations. It would start with enough vaccines to immunize the 3% of its highest-risk population, especially front-line health and social care workers. Additional doses would then be given, until immunization covers 20% of the population in each country, starting with those most at risk of COVID-19, such as the elderly and people with comorbidities.
Phase 2: Vaccines would be delivered to specific countries based on how fast the virus is spreading, whether other pathogens (such as measles) are also spreading, and the vulnerability of the country's health infrastructure. Given the existing limitations, the BioNTech-Pfizer vaccine, for example, must be given in two doses three weeks apart, with only 1.35 billion doses to be produced, at the most, by the end of this year.
However, although the United States did not join because of former US President Donald Trump's "America First" approach, his successor, Joe Biden, promised that the United States will contribute $ 4 billion to COVAX. This was said in the Special Edition of the Conference on Security held from Munich, Germany, with the participation of the Chancellor of that country, Angela Merkel; the President of France, Emmanuel Macron; and the Secretary General of the UN, António Guterres.
The WHO, through COVAX, decided to reserve between 1 and 2.5 million AstraZeneca vaccines for Venezuela, as reported by the head of the mission of the Pan American Health Organization (PAHO) in Venezuela, Paolo Balladelli, who added that it was necessary for the country to pay before February 9 for them to arrive at the end of that month.
It is unknown if the country has been able to pay them since the mechanisms are blocked by unilateral coercive measures applied by the United States and the EU itself. However, the same official has reported via Twitter the installation of the National Table for Access to the COVAX Strategy made up of political, technical and academic actors from Venezuela.
INTELLECTUAL PROPERTY OR COMMODIFICATION OF HEALTH?
Rich countries continue to oppose the South African-Indian proposal to temporarily suspend the relevant provisions of the 1994 World Trade Organization (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) to effectively block the rapid increase in the production of generic vaccines.
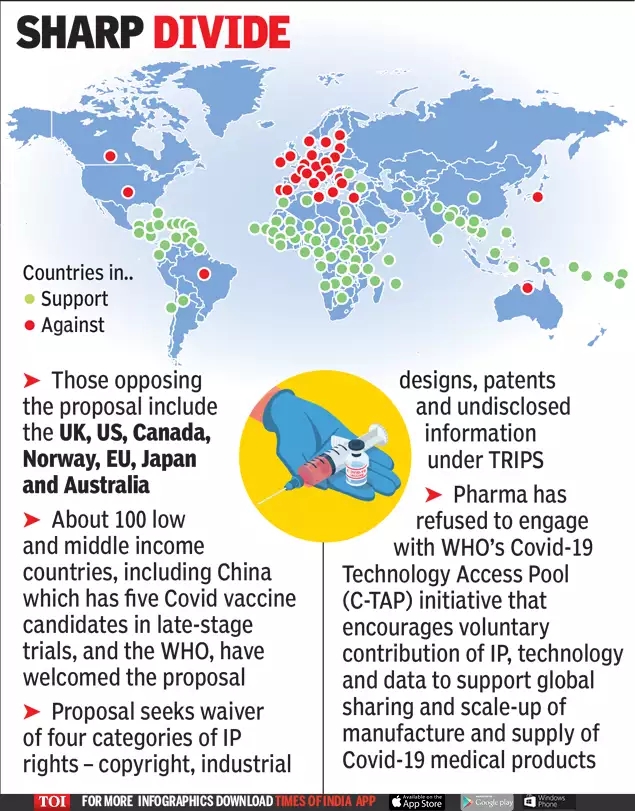
The United Kingdom, the United States, Canada, Norway, the European Union, Japan, Brazil and Australia oppose the development of generic anticovid vaccines that allow greater accessibility and speed of distribution that prevent more infections, infections, deaths (Photo: Times of India)
This refusal, which is due to the maximization of the benefits of vaccine providers, limits supply and access for poor countries; while the rich will be able to vaccinate their residents several times due to their excessive purchases.
Vaccines produced generically (without associated brands) on a larger scale would be much more affordable and infections, infections, deaths and disorders would be stopped more quickly until herd immunity is achieved at national, regional and global levels, depending on the most urgent need.
Big pharma keeps the results of their research secret, which centralizes and restricts vaccine production remains in their hands. If they shared their vaccine with other producers, faster distribution would be possible.
The transnational application of intellectual property rights (IPR) is relatively recent, in 1994 big pharmaceuticals pressured their governments to include TRIPS in the founding documents of the WTO.
Today, while not very transparent agreements are disputed, European politicians threaten to "hoard patents". EU President Charles Michel has warned of the adoption of "urgent measures" to require the granting of compulsory licenses , provided for in the European Treaty.
With such a measure, big pharma would facilitate the production of generic vaccines, something that the TRIPS temporary exemption proposal, supported by developing countries, seeks for all countries. However, the EU and other rich countries are opposed to speeding up supply in this way.
Last May, a team of prominent Finnish researchers had a patent-free vaccine against covid-19 ready, which they have dubbed "the Linux of vaccines", with it they could have been allowed to countries around the world. world to inoculate their populations without having to pay a lot of money, but Finland chose to rely on big pharma putting their profits above public health.
To accelerate vaccine development, the costs and risks have been borne primarily by governments, rather than by developers or private funding. The top six candidate vaccine developers have already received more than $ 12 billion of public money, sometimes with little to show.
The American transnational Moderna received $ 955 million for R&D, in addition to a pre-market purchase commitment of $ 1.530 million. In Europe, Pfizer / BioNTech obtained 375 million euros from the German government and another 100 million for the refinancing of the debt of the European Investment Bank.
Even though they receive massive public funding, the big vaccine pharmas retain the monopoly right of intellectual property to obtain revenues that, just from the sale of vaccines in 2021, amount to almost 40 billion dollars while the expectations that the pandemic stop killing people would remain for a few years, apparently.
Left: Research Division. Center: Profit division. Right: Elimination of affordable generics (Photo: Archive)
***
Taxpayers are paying up to three times for each vaccine: first for its development in academic institutions maintained with taxes administered by governments, then for the finished product and, if we had to take responsibility for the possible side effects of the coronavirus vaccines , governments are obliged to pay compensation.
The never ending story between large corporations and states: profits are private, risks are socialized.
https://misionverdad.com/globalistan/bi ... a-el-covid
Google Translator
How long Lord, how long?
Eder Peña
4 Mar 2021 , 11:39 am .
Big Pharma, spoiled companies of capitalism (Photo: The Motley Food)
By mid-February, the global pandemic had infected at least 109 million people worldwide and caused more than 2.4 million deaths after a year. Its effects have cost 28 trillion dollars in production losses worldwide, and developed countries would have contracted economically by 7% in 2020.
One of the critical issues that has not made it possible to overcome the pandemic, in addition to the contradictions evidenced (one by one) of global capitalism, has to do with the slowness in the development and distribution of preventive covid-19 vaccines.
When talking about "slowness", one might think that it is only a question of criticizing the time it took for pharmaceutical companies to develop and test vaccine candidates, but the issue goes deeper: Since the SARS outbreak in 2002, another coronavirus, several Scientific sectors repeatedly warned about the risk of a pandemic but the big pharmaceutical companies (Big Pharma) refused to do any research on it because there were no expectations of profits at the time.
Even in 2016 the World Health Organization (WHO) placed coronaviruses among the eight main viral threats that required more investigation, the result is known: Last year we were not prepared for the arrival of SARS-CoV-2.
This and other avoidable delays in preventive vaccination (as the most effective measure) are imposing burdens on the global economy and human well-being in a context where economic upheavals demand more relief and recovery measures as powers play at self-preservation.
BIG PHARMA, SPOILED BY CAPITALISM
The capital of the pharmaceutical industry is concentrated in ten companies, this is greater in the production of vaccines because almost all the knowledge is in the hands of GSK, Johnson & Johnson, Pfizer and Sanofi.
Almost all Research and Development (R&D) is done in government and university laboratories paid for by taxpayers, and the sector also has tax credits and other financial concessions to cover possible risks. As drugs are developed, these companies can patent them and both consumers and governments are then charged high prices.
Their profit margins are appreciably higher across all industries, speaking of a yield of 17.3 percent compared to an average of 11.5 percent in the rest. They tend to "forget" to pay taxes on their soaring earnings to the point that only the first four big pharma evade $ 3.8 billion in taxes a year, according to the NGO Oxfam .
It would be possible to defend them if those super earnings were used for innovation and investments but they spend more on paying dividends and buying back their own shares than on R&D. Also, almost a fifth of all profits go to marketing and advertising .
Most Big Pharma invests more in sales and marketing than in research and development because the latter is done by governments (Photo: Statista)
Finally, of all the research and development in Europe, only one tenth is truly innovative. The other 90% are so-called "imitation drugs" (in English "me-too drugs") or drugs that make small changes to an existing drug.
By the end of 2020, Pfizer had sold more than 80% of the vaccine doses it could produce by the end of 2021 to governments representing 14% of the world's population. In other words, if this had been the first safe and effective vaccine to hit the market, the vast majority of the world's population would have had almost no access to it.
PFIZER AND ITS HIGH-LEVEL BULLYING
The big pharma Pfizer has entered, again, the media controversy because The Bureau of Investigative Journalism (TBIJ) published a report in which it is accused of bullying (intimidation) to, at least, three Latin American governments in the Covid vaccine negotiations and has asked some countries, such as Argentina and Brazil, to put up sovereign assets, such as embassy buildings and military bases, as collateral against the cost of any future legal cases.
In neither case was a national agreement reached, even though such delays in receiving vaccines by countries mean more infections and, consequently, more deaths.
In the case of another country, whose name is hidden by the authors of the report, the demands of the big pharma caused a delay of three months in the agreement on vaccines. Pfizer has held talks with more than 100 countries and supranational organizations, in Latin America and the Caribbean it has reached agreements, the terms of which are unknown, with Chile, Colombia, Costa Rica, the Dominican Republic, Ecuador, Mexico, Panama, Peru and Uruguay.
Pfizer negotiators demanded that recipient countries pay the potential costs of civil lawsuits that arise as a result of the company's own acts of negligence, fraud or malice if the vaccines caused injury, disability or death after being inoculated. This was described as "high-level intimidation" by an official who was present at the negotiations in the unidentified country.
Spending on lobbies (pressure) in the United States reached almost 3.5 billion dollars in 2019, the highest in 9 years, Big Pharma (health) were the ones that spent the most (Photo: Statista)
For its part, Pfizer told TBIJ that "Globally, we have also allocated doses to low- and lower-middle-income countries at a non-profit price, including an advance purchase agreement with Covax to provide up to 40 million doses in 2021. We are committed to supporting efforts to provide developing countries with the same access to vaccines as the rest of the world, "declining to comment on the ongoing private negotiations.
As the manufacturers have developed vaccines quickly and because they protect all members of society, governments usually agree to cover the cost of compensation and, thus, if a citizen who suffers an adverse effect after being vaccinated can present a claim against the manufacturer and, if successful, the government would pay the compensation.
This places an additional burden on some countries, as it means having to hire specialized lawyers and, at times, pass complex new legislation, in order to exempt manufacturers from their responsibilities.
In the case of Argentina, an official told TBIJ that Congress approved a new law in October that allowed it, but that was not enough for Pfizer, it was not happy with the drafting of the legislation because the government believed that they should take responsibility for it. any act of negligence or malice.
The government offered to amend the existing law to make it clear that "negligence" meant problems in the distribution and delivery of vaccines (inadvertent interruption of the vaccine's cold chain, for example), but Pfizer remained dissatisfied. He asked the government to modify the legislation through a new decree and President Alberto Fernández refused.
In late December, Pfizer asked the government to put up sovereign assets such as federal bank reserves, embassy buildings or military bases as collateral. One of the reasons the government wanted Pfizer's vaccines was because the company said they could be delivered quickly. However, in the contract, Pfizer wanted to reserve the right to change the schedule. There was no room for negotiation.
APARTHEID AND THE GLOBAL FUNNEL LAW
In a world in which elites privilege the disappearance or minimization of states, the pharmaceutical business consists of financing governments to research and develop vaccines and shifting the possible costs of adverse effects onto ... governments , this includes low- and middle-income countries.
This is how BioNTech, a partner of Pfizer, received 445 million dollars from the German government to develop a vaccine, and the US government agreed last July to an agreement to pre-order 100 million doses for almost 2 billion dollars, before the vaccine would have even entered phase three of the trials. Pfizer expects to sell $ 15 billion worth of vaccines in 2021, 7.5 times more.
But the development of the vaccine is one thing, its production and distribution is another. Marc Vandepitte says that vaccine manufacturers have little interest in rapidly and massively increasing their own production capacity. Increasing the production capacity in six months would leave the new infrastructure empty instantly because the profitable business consists of the current: That the existing factories produce for years at their current capacity.
By the end of 2021, the total global capacity of the top 13 COVID-19 vaccine manufacturers would still be well below the needs of the world's nearly 7.7 billion people. Even if everyone produces to the maximum of their capacity, a fifth of the world's population would not have access until 2022.
There is a kind of apartheid to more than 85 poor countries that will not have public access to vaccines before 2023 due to patent protections, limitations on vaccine production and the accumulation of rich countries. Until last February 5, not a single dose had been administered in 130 countries with 2.5 billion people.
Of the more than 131 million doses available as of February 8, the United States, China, the European Union and the United Kingdom had 78% while Africa had 0.2%. The African Union (AU) has only asked for 670 million doses, less than half of what it needs to achieve herd immunity. In addition to Brazil, other Latin American countries only have 150 million doses for less than a quarter of their population.
Doses of anticovid vaccines administered per 100 people in various countries since last January (Photo: Our world in data)
Global needs far exceed available supply, and middle-income countries have joined the struggle by making direct and non-transparent deals with vaccine suppliers, usually in worse conditions than if they had bargained collectively. Divided and naturally out-of-date, it's no wonder that vaccine prices vary considerably, by more than 12 times, from $ 6 to $ 74 per dose.
This so-called "vaccine imperialism" contrasts with the "vaccine nationalism" that the great powers apply to themselves, this chapter the law of the global funnel deals with how, after its dispute with AstraZeneca , the European Commission (EC) banned the vaccine exports to most countries outside the EU.
Even though the AstraZeneca vaccine was "tested" in the South African population, this country is paying 2.4 times more than the EU: $ 5.25 versus $ 2.16. Gone was the promise of "benefit sharing" and "priority access after the trial", much further for Uganda, which is paying 20% more than South Africa.
VACCINES FOR EVERYONE?
The Global Covid-19 Vaccine Access Mechanism (COVAX) is led by WHO, the Coalition for Innovations in Epidemic Preparedness and the Alliance for Vaccines (Gavi) and aims to accelerate vaccine development, ensure doses for all countries and distribute it fairly, starting with the highest risk groups.
Although it was created, in part, to prevent hoarding by the governments of rich countries, and so far more than 180 countries, representing almost two-thirds of the world's population, have joined, the results are obvious.
Among the 180 countries are 94 high-income countries that have made legally binding commitments. Everyone will have access to the vaccines on the COVAX list, and will pay for their doses individually. The 92 lower-income countries that are part of the device will receive their doses for free.
The COVAX plan consists of two phases:
Phase 1: All participating countries would receive doses proportional to their populations. It would start with enough vaccines to immunize the 3% of its highest-risk population, especially front-line health and social care workers. Additional doses would then be given, until immunization covers 20% of the population in each country, starting with those most at risk of COVID-19, such as the elderly and people with comorbidities.
Phase 2: Vaccines would be delivered to specific countries based on how fast the virus is spreading, whether other pathogens (such as measles) are also spreading, and the vulnerability of the country's health infrastructure. Given the existing limitations, the BioNTech-Pfizer vaccine, for example, must be given in two doses three weeks apart, with only 1.35 billion doses to be produced, at the most, by the end of this year.
However, although the United States did not join because of former US President Donald Trump's "America First" approach, his successor, Joe Biden, promised that the United States will contribute $ 4 billion to COVAX. This was said in the Special Edition of the Conference on Security held from Munich, Germany, with the participation of the Chancellor of that country, Angela Merkel; the President of France, Emmanuel Macron; and the Secretary General of the UN, António Guterres.
The WHO, through COVAX, decided to reserve between 1 and 2.5 million AstraZeneca vaccines for Venezuela, as reported by the head of the mission of the Pan American Health Organization (PAHO) in Venezuela, Paolo Balladelli, who added that it was necessary for the country to pay before February 9 for them to arrive at the end of that month.
It is unknown if the country has been able to pay them since the mechanisms are blocked by unilateral coercive measures applied by the United States and the EU itself. However, the same official has reported via Twitter the installation of the National Table for Access to the COVAX Strategy made up of political, technical and academic actors from Venezuela.
INTELLECTUAL PROPERTY OR COMMODIFICATION OF HEALTH?
Rich countries continue to oppose the South African-Indian proposal to temporarily suspend the relevant provisions of the 1994 World Trade Organization (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) to effectively block the rapid increase in the production of generic vaccines.
The United Kingdom, the United States, Canada, Norway, the European Union, Japan, Brazil and Australia oppose the development of generic anticovid vaccines that allow greater accessibility and speed of distribution that prevent more infections, infections, deaths (Photo: Times of India)
This refusal, which is due to the maximization of the benefits of vaccine providers, limits supply and access for poor countries; while the rich will be able to vaccinate their residents several times due to their excessive purchases.
Vaccines produced generically (without associated brands) on a larger scale would be much more affordable and infections, infections, deaths and disorders would be stopped more quickly until herd immunity is achieved at national, regional and global levels, depending on the most urgent need.
Big pharma keeps the results of their research secret, which centralizes and restricts vaccine production remains in their hands. If they shared their vaccine with other producers, faster distribution would be possible.
The transnational application of intellectual property rights (IPR) is relatively recent, in 1994 big pharmaceuticals pressured their governments to include TRIPS in the founding documents of the WTO.
Today, while not very transparent agreements are disputed, European politicians threaten to "hoard patents". EU President Charles Michel has warned of the adoption of "urgent measures" to require the granting of compulsory licenses , provided for in the European Treaty.
With such a measure, big pharma would facilitate the production of generic vaccines, something that the TRIPS temporary exemption proposal, supported by developing countries, seeks for all countries. However, the EU and other rich countries are opposed to speeding up supply in this way.
Last May, a team of prominent Finnish researchers had a patent-free vaccine against covid-19 ready, which they have dubbed "the Linux of vaccines", with it they could have been allowed to countries around the world. world to inoculate their populations without having to pay a lot of money, but Finland chose to rely on big pharma putting their profits above public health.
To accelerate vaccine development, the costs and risks have been borne primarily by governments, rather than by developers or private funding. The top six candidate vaccine developers have already received more than $ 12 billion of public money, sometimes with little to show.
The American transnational Moderna received $ 955 million for R&D, in addition to a pre-market purchase commitment of $ 1.530 million. In Europe, Pfizer / BioNTech obtained 375 million euros from the German government and another 100 million for the refinancing of the debt of the European Investment Bank.
Even though they receive massive public funding, the big vaccine pharmas retain the monopoly right of intellectual property to obtain revenues that, just from the sale of vaccines in 2021, amount to almost 40 billion dollars while the expectations that the pandemic stop killing people would remain for a few years, apparently.
Left: Research Division. Center: Profit division. Right: Elimination of affordable generics (Photo: Archive)
***
Taxpayers are paying up to three times for each vaccine: first for its development in academic institutions maintained with taxes administered by governments, then for the finished product and, if we had to take responsibility for the possible side effects of the coronavirus vaccines , governments are obliged to pay compensation.
The never ending story between large corporations and states: profits are private, risks are socialized.
https://misionverdad.com/globalistan/bi ... a-el-covid
Google Translator
How long Lord, how long?
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis

The political economy of COVID-19 vaccines
Posted Mar 09, 2021 by Jayati Ghosh
Originally published: The Indian Forum (March 5, 2021) |
The COVID-19 pandemic has been unusual in several ways: the disproportionate extent to which people in rich countries (particularly in Europe and North America) have been affected; the sheer scale of the policy response for containment; and the speed and urgency of the global response.
The active interest in controlling the pandemic in rich countries shaped individual national responses as well as global policy. There was a massive push for vaccine development, through large subsidies for research and development to drug companies, pre-orders of vaccines, and other support by the US, Russia, China, and European countries.
This led to the rapid development of multiple COVID-19 vaccine candidates and even more rapid regulatory approval to several of them. Typically, vaccines take several years to be developed and approved, partly because of extended clinical trials to check for all possible responses. But some COVID-19 vaccine candidates were given official approval in Russia and China even before the essential Phase III trials were completed. Even in the U.S. and Europe, regulatory processes were accelerated, sweeping aside the usual demands for complete data and without checking for possible side effects.
Despite such proactive policy, the production and distribution of COVID-19 vaccines has exposed and intensified global inequality. Three features stand out: blatant vaccine grab by rich countries; protection of patent rights by governments in advanced countries, which prevents wider production of vaccines; and the use of vaccine distribution to promote both nationalism and diplomatic ‘soft power’.
The great vaccine grab
It seems obvious that a pandemic can be overcome only when it is overcome everywhere. The delayed vaccination of people across the world increases the possibility of virus mutation, reducing the ability to control the pandemic even in rich countries that have bagged vaccines. Prolonged fear of infection, because of inadequate vaccination, affects economic prospects, inhibiting and delaying global economic recovery. These risks are so great that rich countries would still benefit even if they decided to pay on their own for vaccinating all of the world’s population.
An ‘every-country-for-itself’ approach is irrational and even counterproductive. Yet that is exactly what has happened.
When three major vaccine candidates (from Pfizer-BioNTech, Moderna, and AstraZeneca) were approved in the U.S. and Europe, rich countries scrambled to lay claim to vaccine doses, confirming that wealthy countries and individuals would monopolise early doses of any effective vaccine. As a result, by late February 2021 COVID-19 vaccinations were heavily concentrated in the developed world (Figure 1).
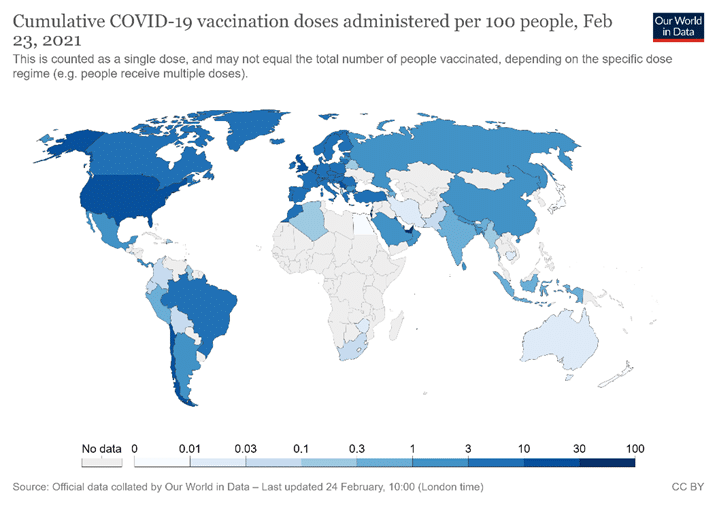
Figure 1. Source: Coronavirus (Covid-19) Vaccinations. Accessed on 24 February 2021
This need not have occurred. The COVID-19 Vaccines Global Access Facility (COVAX) led by the World Health Organisation (WHO), the Coalition for Epidemic Preparedness Innovations, and Gavi, was established precisely to prevent this outcome, to prevent hoarding by rich countries and ensure access for the world’s poor. COVAX aims to accelerate COVID-19 vaccine development, secure doses for all countries, and distribute those doses fairly, beginning with the highest-risk groups. By early 2021, 190 countries, representing most of the world’s population, had joined. In February, the United States (which had been kept out by former president Donald Trump) also joined. Higher-income and middle-income countries will have access to the vaccines in the COVAX list and pay for their doses individually. The 92 lower-income member countries are to receive their doses free of charge.
The COVAX plan is to distribute vaccines in two phases. In the first phase, all participating countries would receive doses proportionate to their populations, beginning with enough doses to immunise the 3% of their population at highest risk, especially frontline workers in health and social care. Additional doses would then be delivered to cover 20% of each country’s population, beginning with others most in danger, such as the elderly and those with co-morbidities. In the second phase, vaccines would be delivered to specific countries based on how quickly the virus is spreading; whether other pathogens (like measles) are also spreading; and how vulnerable the country’s health infrastructure is to being overwhelmed. Eventually, everyone would be covered.
This is a fair system, given constraints on production. But the facility still remains underfunded, thus far raising only $4 billion of its modest target of $6.8 billion for 2021. Even worse, it has not been able to purchase the vaccines required for free distribution to poor countries as much as planned. This is because the COVAX facility allows member countries to make their own separate purchases directly from pharma companies. As a result, rich countries have competed to secure bilateral deals with pharmaceutical companies outside of COVAX. Within a month of the regulatory approval being granted to the first three vaccines, advanced countries, accounting for only 14% of the world’s population, had placed orders for around 85% of the estimated entire production for 2021 (Ghosh 2020).
Much of this was in the form of pre-orders even before regulatory approval was granted. Thirteen of the 48 firms engaged in COVID-19 vaccine development had made advance sales by mid-November 2020, promising to deliver 7.5 billion doses of vaccines, mostly to advanced countries, even before emergency-use authorisation had been granted. In some cases, this happened even before the clinical trials necessary for regulatory approval had been completed (Acharya and Reddy 2021).
Forty-four bilateral deals between governments and pharmaceutical companies (dominated by rich countries) were signed last year, and at least 12 have already been signed this year. Canada has ordered vaccines that could provide for more than 10 times its population–and then sought to get vaccines from COVAX as well. The U.S. has ordered vaccines equivalent to more than four times its population. Rich countries are now stockpiling vaccines that they have grabbed but are unable to distribute. Firms preferred to sell in these bilateral deals because they could charge higher prices than offered by COVAX. They typically keep secret the basic elements of the deal, including the price at which the vaccines were being provided to these governments.
This vaccine grab by rich countries meant that most of the world would get safe and approved vaccines only in 2022, and in some cases not even until 2024. In mid-January 2021, the head of the WHO noted that while 39 million vaccine doses had already been administered in the rich countries, in one poor country only 25 doses (in total) had been given, and 170 poorest countries had received no vaccines at all. He said: “I need to be blunt: the world is on the brink of a catastrophic moral failure–and the price of this failure will be paid with lives and livelihoods in the world’s poorest countries” (UN News, January 2021).
The unjustified protection of intellectual property
Insufficient production is an important reason for the poor and unequal distribution. Yet this scarcity is completely unnecessary and could be easily and rapidly remedied. The major factor limiting supply of approved vaccines is the persistence of patent rights that give pharmaceutical companies a monopoly on production, confining supplies to their own capacities and the few production licences they choose to issue to others.
Patents are usually seen as providing a necessary financial reward for invention/innovation, without which technological change would either not occur or be more limited. Big pharma (which has been the major lobby pushing for inclusion of intellectual property rights in the World Trade Organization (WTO) and in subsequent trade and economic partnership agreements) argues that developing new drugs requires such incentives because the costs are very high and drugs may not succeed even after years of effort.
Yet for COVID-19 vaccines, many big pharma companies received massive subsidies from governments that have mostly and in some cases completely covered research and development costs. In the U.S. alone, the six major vaccine companies received over $12 billion in public subsidies for developing COVID-19 vaccines (MSF 2021). Other rich country governments have provided similar subsidies. Private pharma companies also benefited from prior public research (Scientific American 2020) and reduced costs of clinical testing, because of more unpaid volunteers for trials. The ‘leader’ vaccines may have already received what could be considered as reasonable returns on their own investment, and more. For example, while Pfizer did not receive direct subsidies from the U.S. government, I received pre-orders for 100 million doses for $1.95 billion (Industry Week 2020). Moreover, it relied on technology from BioNTech, which had received $445 million from the German government for their research (Bloomberg 2020). Pfizer claims costs of $3.1 billion to develop this vaccine (BBC 2020), while estimated sales in 2021 will be worth $15 billion (Quartz, 2020). Developing the Moderna vaccine cost $2.5 billion, apparently entirely funded by the U.S. federal government (USA Today, 2020). The recently approved Johnson and Johnson vaccine benefited from U.S. government subsidies and a pre-order of 100 million doses likely to cover costs (Johnson and Johnson 2020).
The case of the AstraZeneca vaccine is particularly instructive, also because it is seen as viable for developing country use. (Significant quantities of this vaccine are being produced by the Serum Institute of India under a collaboration agreement.) The vaccine was entirely developed by a publicly funded lab at Oxford University. The original distribution model was for an open-licence platform, designed to make the vaccine freely available for any manufacturer. However, the Gates Foundation, which had clout because it had donated $750 million to Oxford for vaccine development, persuaded the university to change course completely and sign “an exclusive vaccine deal with AstraZeneca that gave the pharmaceutical giant sole rights and no guarantee of low prices” (Jay Hancock 2020).
Oxford and AstraZeneca promised not to make profits from sale of the vaccine, but the details were left vague. While Oxford will receive no royalties during the pandemic, it could subsequently gain from patents including those held by Vaccitech, a for-profit spinoff.
Meanwhile, AstraZeneca is charging differential prices for its vaccines sent to different countries, with some poorer countries paying higher rates. The European Union pays $3.50 per dose, while Bangladesh pays $4, and South Africa as much as $5.25 (Politico, 2021). (The more expensive vaccines are being provided by the Serum Institute of India.)
This variation in prices is not confined to the AstraZeneca shot. Because of competition for doses and opacity in contracts, the range of reported prices of vaccines is vast: from $2.19 to as much as $44 per dose, as of 1 March. (UNICEF, Covid Dashboard).
This restricted production creating unseemly vaccine grabs, overpriced and differentially priced doses determined by private suppliers, and inadequate provision for most of the world’s population, could all have been avoided if a proposal brought by India and South Africa to the WTO in October 2020 had been accepted. The proposal was for a waiver of obligations to enforce patents and other intellectual property rights related to COVID-19 products (MSF, November 2020).
This would mean that WTO members could choose not to grant or enforce patents and other intellectual property related to all COVID-19 drugs, vaccines, diagnostics, and other technologies, including masks and ventilators, for the duration of the pandemic. They could also more easily collaborate in research and development, technology transfer, manufacturing, scaling up, and supplying COVID-19 tools.
Most developing countries have supported this, but advanced countries have repeatedly blocked it in the TRIPS council of the WTO (Prabhala et al 2020). This is surprising, because such suspension would also benefit populations in the advanced countries by making available more vaccines quickly. A larger supply would reduce costs of additional vaccines, making them cheaper for governments and taxpayers across the world.
The blocking of the proposal at the WTO is presumably because of the lobbying power of multinational pharma companies, which have thus far been successful in preventing the TRIPS council from approving this on five separate attempts. (Incidentally, Bill Gates has refused to back this proposal (Mail & Guardian 2021).
Figure 2 indicates how responses to this proposal in the WTO have closely tracked the persistent divide between global North and South. Rich countries that are home to the major multinational pharma companies have blocked it. These countries have already secured more than their requirements of COVID-19 vaccines. (It is a different matter that most of them have been less successful in distributing them quickly within their own countries, so they are now stockpiling vaccines.)
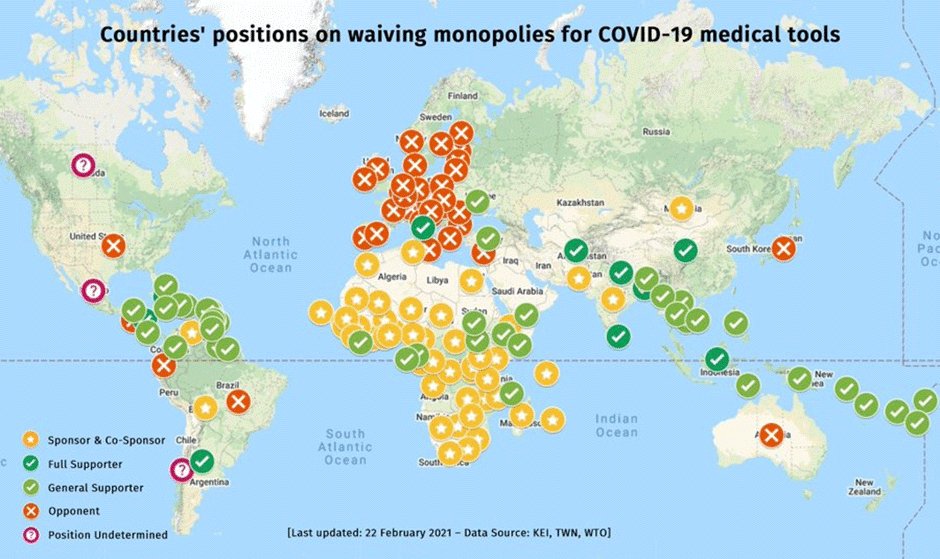
Figure 2. Source: Medecins san Frontiers, accessed 21 February 2021
Some have argued that this proposal is not necessary, since the WTO agreement on TRIPS already allows for compulsory licensing. The 2001 Doha Declaration on TRIPS and Public Health explicitly mentions public health emergencies as adequate cause to issue compulsory licences. A compulsory licence is an authorisation granted by a government to a third party to produce a patented product or process, without the express consent of the patentee (See WTO FAQs). It allows a government to override the patentee’s exclusive right to keep others from using its patented inventions. The idea is to prevent monopolistic behaviour, like preventing others from producing and charging excessively high prices. Conditions for compulsory licencing are obviously met in this pandemic, which is clearly a public health emergency. Some countries, like Chile and Israel, have already passed resolutions for such licences to be issued in the wake of the pandemic.
However, the difficulty with issuing compulsory licences in individual developing countries is that the transfer of technology by the inventor to other licenced producers is not compulsory. For pharmaceuticals, if the chemical composition of the product is known, the product can be reverse engineered and produced by other companies. When the precise technology for producing the vaccine is not known, compulsory licencing works only when patent holders are willing to make available the technology to licenced producers. In the case of COVID-19 vaccines, the big pharma companies are happy to supply rich countries that are already competing for privileged access to the limited vaccine supply, and therefore are not really concerned about access to smaller or less well-endowed markets. A global waiver would change those incentives for companies.
Therefore, a global move for suspension and/or modification of intellectual property rights for matters relating to essential public health concerns is essential. Since there is as yet no information on the immunity period offered by most of the vaccines, the suspension might be required for a more extended period. Such exemptions would be required not just for vaccines but for other treatments, tests, and products related to the pandemic, which may be required for the next few years.
Another idea is that of “voluntary pooling”, proposed by Costa Rica and supported by the WHO, which has created the COVID-19 Technology Access Pool (CTAP). This creates a pool of rights to tests, medicines and vaccines, with free access or licensing on reasonable and affordable terms for all countries. But so far only 40 (developing) countries have joined, and the major players have kept away. Lack of international support has meant that CTAP is not really effective thus far–but it may become significant in future, extending beyond the current COVID-19 pandemic to health emergencies in the future.
Regulatory approval and public trust
Other vaccine candidates being developed elsewhere also have the potential to combat the pandemic and ease the current shortages. The Sputnik V vaccine developed in Russia and the Sinovac and Sinopharm vaccines developed in China are reportedly effective. There are other vaccines being developed in India, Cuba, and elsewhere. Some have concerns about inadequate testing and hasty regulatory approval without the required trials and other processes. But even when these vaccine candidates are found to be safe and effective through clinical trials, there are further hurdles to their being accepted internationally.
This is largely because the WHO’s approval process is heavily skewed in favour of vaccines developed in the rich countries. The WHO has a list of ‘stringent regulatory authorities’ it trusts for quality control, which are only from developed countries in Europe, the US, Canada, Australia, and Japan. For the rest of the world, vaccine (and other drug) candidates are required to go through ‘prequalification’— a much more complicated and extended process. This greatly prolongs the time taken before vaccines from other countries are approved.
For example, the WHO approved the Pfizer-BioNTech vaccine at the end of 2020, less than two months after application, because WHO collaborates with the European Medicines Agency (EMA). However, the Russian (Sputnik) and Chinese (Sinovac and Sinopharm) vaccines, which had applied for approval even before the Pfizer-BioNTech vaccine, have still not received the WHO approval (Prabhala and Ling, 2021). All three of these companies can each produce up to 1 billion doses of vaccine in 2021 and have licensed production to other producers in developing countries.
In this pandemic, the usual regulatory standards have been greatly relaxed across the world, including in developed countries. No COVID-19 vaccine has been developed or released as transparently as it should have been. Even if WHO feels the regulatory standards in other countries might be less stringent, it could still work with different national regulatory authorities to ensure that all vaccine candidates are treated on an equal footing. Given the global scarcity that is denying people in poor countries access to vaccines, the WHO should take a proactive approach to enable global distribution of such vaccines when they meet some harmonised standards.
If this is done, it may be possible to circumvent the stranglehold of the big pharma companies on COVID-19 vaccines, which enables private profiteering in the midst of a health crisis and widespread economic distress. Some countries have already approved these other vaccine candidates for domestic use and have benefited from this access.
For example, by late February 2021 Chile had managed to provided vaccine doses to 17% of its population, by relying on imports of the China’s Sinovac, which is also being used in Bolivia, Brazil, Indonesia, and Turkey. Several countries have approved the Sinopharm vaccine, including UAE, Bahrain, Egypt, Jordan, Iraq, Serbia, Morocco, Hungary, and Pakistan. The Sputnik V vaccine is likely to be produced and distributed in several countries across Europe, the Middle East, Africa, and Latin America.
India should have been a prime example of successful production and distribution of COVID-19 vaccines. It has a number of major vaccine companies, has a long and successful history of inoculation drives, and until recently, there was a high degree of public trust in vaccines. Unfortunately, over-enthusiastic attempts by the government to first promote and then push particular vaccine candidates (Covaxin produced by Bharat Biotech) even before the required clinical trials were completed may have proved to be counterproductive, reducing public trust within and outside India. There have been many reports of people in India–including health workers–refusing to be vaccinated with Covaxin.
This is unfortunate, since once such trust has been lost, it takes time to be remedied and reversed. It also has an impact on India’s ability to export vaccines now and in the future. A recent YouGov poll of 19,000 people in 17 developed countries found that vaccines developed in Russia, China, and India ranked lowest in popular perceptions of efficacy, just above Iran which has very little vaccine production (Prabhala and Ling, 2021). India has also been plagued by major issues in distribution, belying expectations and past experience of vaccination drives.
To be fair, most countries have shown poor performance in vaccine rollout, including the developed countries that have sought to grab many multiples of their required shares of global supply. Overall, domestic distribution of vaccines has mostly mirrored the global distribution: unequal, unjust, and incompetent. This approach will delay the resolution of the ongoing pandemic and creates concerns about humanity’s ability to co-operate to address with the even greater challenges ahead.
https://mronline.org/2021/03/09/the-pol ... -vaccines/
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis
CAPITALISM, GEOPOLITICS AND PANDEMIC
Sergio Rodríguez Gelfenstein
11 Mar 2021 , 11:11 am .

A man walks with his purchases next to a wall painting depicting a person wearing a gas mask in Milan on March 16, 2020 (Photo: AAP)
With great fanfare it was announced a few months ago that the end of the pandemic would mean a "new beginning", something quite undefined that obviously for Latin America will no longer occur in 2021 since the mutation of the virus has produced novel variants that have Brazil as its most recognized epicenter in the face of the WHO alarm that has declared a health emergency for the entire region.
On the other hand, so far vaccination in Latin America and the Caribbean reaches 2.8% of its population, while in the world it reaches 3.5%. That figure is very low if we consider that the population of the region is 8.1% of the planet's total. This shows how the inoculation process has been concentrated in very few countries.
Perhaps no event in the history of the last 250 years such as the management of the pandemic and in particular the production and distribution of vaccines to counteract the virus, has demonstrated with such transparency the true spirit of capitalist society.
For those who still cannot determine the insignificant importance that human life and peace have for transnational companies and capitalist powers, it is enough to review the conditions that are imposed for the supply of vaccines.
The US pharmaceutical company Pfizer has been known to intimidate Latin American governments in negotiations to sell them the COVID-19 vaccine. Pfizer required some countries to put sovereign assets, such as embassy buildings and even military bases, as collateral to reimburse the costs of any future litigation.
These requirements imposed in the "negotiation" led Argentina and Brazil to refuse to buy the vaccine from this company. However, the agreements to obtain it are covered by confidentiality clauses that have been made public by the scandal that means that Pfizer forced a series of damages against civil claims, both for adverse effects of the vaccine and for its own negligence.
Thus, the US company requires governments to pay the potential costs of civil lawsuits that may be initiated due to negligence, fraud or malice. This includes the guarantee of the companies that are covered in the event that under their responsibility the cold chain is interrupted, the wrong vaccines are delivered or if they are damaged. Also, if death, disability or an associated disease is caused to the patient. In other words, it is the governments that must pay for the errors of the companies if the former file a formal claim in court.
These conditions that put the interests of companies in the first place and in the background the health of citizens were accepted by Chile, Colombia, Costa Rica, the Dominican Republic, Ecuador, Panama, Peru and Uruguay governed by the neoliberal right and unfortunately also by Mexico, without knowing the terms of the agreements with certainty.
On the other hand, and in a frankly different attitude, the Ministry of Foreign Affairs of China has announced that its country will continue to promote an equitable distribution of vaccines, putting their safety and efficacy at the forefront, for which it has urged the country's producing companies to carry out research and development of vaccines in strict approval of scientific methods and regulatory requirements.
In the same way, China has pledged to make COVID vaccines a global public goods and has provided or is providing vaccine aid to 53 countries, while Chinese pharmaceutical companies have exported or are exporting the drugs to 27 others. countries, including 11 from Latin America without any type of condition.
CHINA'S GROWING CAPACITY FOR INSERTION IN WORLD PROBLEMS IS STRENGTHENED
In this situation, coloniality and Eurocentrism have permeated debates about the "new normal." For Latin America and in general for the peoples of the South, to speak of it is to rewind the discourse of the domination and control of the powers. In this way, "new normal" is related to a discourse that is typical of the North, its security and stability to the detriment of the South, which is again seen as an obstacle to the achievement of the objectives set by Washington, Brussels or London.
In other words, the concept of "new normal" for some is associated with that of "risk" for them, which implies new methods of control and exploitation for most of the world. To that extent, this idea links the need for survival of the United States and Europe as dominant powers at any cost, including the lives of millions of citizens.
This environment has led to a repositioning of globalization from another perspective since the virus has been installed in all latitudes and longitudes of the planet, showing the putrefaction in the bowels of the system, when regardless of the health of humanity they have concentrated on In 10 countries, more than 90% of the vaccines produced so far, even having in some countries like Canada quantities 5 times higher than the needs of their population.
The globalization of the pandemic made the peoples of the northern countries feel for the first time the misery of the policies of their governments, perceiving the fears, anxieties and daily threats that southern countries experience. This, without reaching the extremes that, for example, express the policies of the United States government that prohibits laboratories -or risk of sanctions- from selling vaccines to Venezuela and preventing the stolen and retained resources of the country from being used to obtain the vaccine.
Today, it is already possible to predict that transcendent changes will occur in geopolitical terms, which, already underway at the beginning of 2020, were accelerated by the pandemic. The most important of all is the strengthening of China's economic potential and its growing capacity for insertion into world problems.
On the other hand, the pandemic has made evident the distance between the periphery and the centers of world power, when these, far from taking advantage of the disastrous event as a humanitarian meeting place to safeguard life through cooperation and encounter, have profit interests that announce a greater deepening of differences in a world in which the capitalist system has shown its total inability to lead the process of confrontation, struggle and defeat of the virus are privileged.
In this context, the multilateral system has revealed notorious imperfections and shortcomings, starting with the actions of the United Nations (UN) itself, which has been unable to manage and lead the process, either due to weakness, subordination or fear. to the fury of the powers and laboratories that see their businesses diminished.
In the same way, the only regional and sub-regional blocs that have been able to articulate joint policies have been the Asians, the rest have been lost in particular attitudes of the governments and in secret agreements that hide complicity, subordination and defense of the large laboratories transnationals. In particular, in this regard, Latin America has been outstanding - once again - in showing the weaknesses of health systems marked by neoliberal practices that expose the visible face of oligarchies that do not skimp on sacrificing lives when it comes to defending their petty interests group or sector.
The truth is that the management of the pandemic, the priorities in the care of citizens to safeguard their lives, the decision on the use of resources of all kinds to face the virus and the production and distribution of the vaccine put on the cover the philosophical foundations on which governments are concerned or not with guaranteeing the right to health and life of all citizens as mandated by the UN Universal Declaration of Human Rights.
https://misionverdad.com/opinion/capita ... y-pandemia
Google Translator
Sergio Rodríguez Gelfenstein
11 Mar 2021 , 11:11 am .
A man walks with his purchases next to a wall painting depicting a person wearing a gas mask in Milan on March 16, 2020 (Photo: AAP)
With great fanfare it was announced a few months ago that the end of the pandemic would mean a "new beginning", something quite undefined that obviously for Latin America will no longer occur in 2021 since the mutation of the virus has produced novel variants that have Brazil as its most recognized epicenter in the face of the WHO alarm that has declared a health emergency for the entire region.
On the other hand, so far vaccination in Latin America and the Caribbean reaches 2.8% of its population, while in the world it reaches 3.5%. That figure is very low if we consider that the population of the region is 8.1% of the planet's total. This shows how the inoculation process has been concentrated in very few countries.
Perhaps no event in the history of the last 250 years such as the management of the pandemic and in particular the production and distribution of vaccines to counteract the virus, has demonstrated with such transparency the true spirit of capitalist society.
For those who still cannot determine the insignificant importance that human life and peace have for transnational companies and capitalist powers, it is enough to review the conditions that are imposed for the supply of vaccines.
The US pharmaceutical company Pfizer has been known to intimidate Latin American governments in negotiations to sell them the COVID-19 vaccine. Pfizer required some countries to put sovereign assets, such as embassy buildings and even military bases, as collateral to reimburse the costs of any future litigation.
These requirements imposed in the "negotiation" led Argentina and Brazil to refuse to buy the vaccine from this company. However, the agreements to obtain it are covered by confidentiality clauses that have been made public by the scandal that means that Pfizer forced a series of damages against civil claims, both for adverse effects of the vaccine and for its own negligence.
Thus, the US company requires governments to pay the potential costs of civil lawsuits that may be initiated due to negligence, fraud or malice. This includes the guarantee of the companies that are covered in the event that under their responsibility the cold chain is interrupted, the wrong vaccines are delivered or if they are damaged. Also, if death, disability or an associated disease is caused to the patient. In other words, it is the governments that must pay for the errors of the companies if the former file a formal claim in court.
These conditions that put the interests of companies in the first place and in the background the health of citizens were accepted by Chile, Colombia, Costa Rica, the Dominican Republic, Ecuador, Panama, Peru and Uruguay governed by the neoliberal right and unfortunately also by Mexico, without knowing the terms of the agreements with certainty.
On the other hand, and in a frankly different attitude, the Ministry of Foreign Affairs of China has announced that its country will continue to promote an equitable distribution of vaccines, putting their safety and efficacy at the forefront, for which it has urged the country's producing companies to carry out research and development of vaccines in strict approval of scientific methods and regulatory requirements.
In the same way, China has pledged to make COVID vaccines a global public goods and has provided or is providing vaccine aid to 53 countries, while Chinese pharmaceutical companies have exported or are exporting the drugs to 27 others. countries, including 11 from Latin America without any type of condition.
CHINA'S GROWING CAPACITY FOR INSERTION IN WORLD PROBLEMS IS STRENGTHENED
In this situation, coloniality and Eurocentrism have permeated debates about the "new normal." For Latin America and in general for the peoples of the South, to speak of it is to rewind the discourse of the domination and control of the powers. In this way, "new normal" is related to a discourse that is typical of the North, its security and stability to the detriment of the South, which is again seen as an obstacle to the achievement of the objectives set by Washington, Brussels or London.
In other words, the concept of "new normal" for some is associated with that of "risk" for them, which implies new methods of control and exploitation for most of the world. To that extent, this idea links the need for survival of the United States and Europe as dominant powers at any cost, including the lives of millions of citizens.
This environment has led to a repositioning of globalization from another perspective since the virus has been installed in all latitudes and longitudes of the planet, showing the putrefaction in the bowels of the system, when regardless of the health of humanity they have concentrated on In 10 countries, more than 90% of the vaccines produced so far, even having in some countries like Canada quantities 5 times higher than the needs of their population.
The globalization of the pandemic made the peoples of the northern countries feel for the first time the misery of the policies of their governments, perceiving the fears, anxieties and daily threats that southern countries experience. This, without reaching the extremes that, for example, express the policies of the United States government that prohibits laboratories -or risk of sanctions- from selling vaccines to Venezuela and preventing the stolen and retained resources of the country from being used to obtain the vaccine.
Today, it is already possible to predict that transcendent changes will occur in geopolitical terms, which, already underway at the beginning of 2020, were accelerated by the pandemic. The most important of all is the strengthening of China's economic potential and its growing capacity for insertion into world problems.
On the other hand, the pandemic has made evident the distance between the periphery and the centers of world power, when these, far from taking advantage of the disastrous event as a humanitarian meeting place to safeguard life through cooperation and encounter, have profit interests that announce a greater deepening of differences in a world in which the capitalist system has shown its total inability to lead the process of confrontation, struggle and defeat of the virus are privileged.
In this context, the multilateral system has revealed notorious imperfections and shortcomings, starting with the actions of the United Nations (UN) itself, which has been unable to manage and lead the process, either due to weakness, subordination or fear. to the fury of the powers and laboratories that see their businesses diminished.
In the same way, the only regional and sub-regional blocs that have been able to articulate joint policies have been the Asians, the rest have been lost in particular attitudes of the governments and in secret agreements that hide complicity, subordination and defense of the large laboratories transnationals. In particular, in this regard, Latin America has been outstanding - once again - in showing the weaknesses of health systems marked by neoliberal practices that expose the visible face of oligarchies that do not skimp on sacrificing lives when it comes to defending their petty interests group or sector.
The truth is that the management of the pandemic, the priorities in the care of citizens to safeguard their lives, the decision on the use of resources of all kinds to face the virus and the production and distribution of the vaccine put on the cover the philosophical foundations on which governments are concerned or not with guaranteeing the right to health and life of all citizens as mandated by the UN Universal Declaration of Human Rights.
https://misionverdad.com/opinion/capita ... y-pandemia
Google Translator
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis

The AstraZeneca / Oxford vaccine has been suspended in several countries around the world, especially in Europe (Photo: Jakub Porzycki / NurPhoto)
THE LUCRATIVE VACCINE DRAMA TAKES THE WORLD BY STORM
Augusto Marquez
15 Mar 2021 , 1:48 pm .
A year ago, when the World Health Organization (WHO) inaugurated the status of a pandemic and death began to plague European and Asian populations, the possibility of an immune solution to the coronavirus was seen as distant. The sensation was of abandonment in a world crowned by inequality and the existential crisis of the capitalist system, a distress that augured worse times.
That is until Pfizer, Moderna and AstraZeneca were presented as a civilizing example of how markets encourage and practice scientific innovation at a critical time for the health of the human species. Very good work of the western media, by the way, pulleys of transmission of the corporate message to the world.
The Big Pharma , once again, won one round in the hopeful hearts and anguish of millions of people worldwide, especially that portion which is able to grab more than 70% of doses available in the market in very few hands. Over the months, the results of the clinical trials of corporate vaccines became known, generating great expectations for business (first) and health (later) in the United States and Europe, while it was discovered that countries such as China and Russia were developing their own vaccines .
Thus began a multipolar race for covid vaccines that generated various strategies:
Pfizer, although it used private funds for the development of its vaccine, benefited from advance and guaranteed orders of 2 billion dollars from the US government and used technology from BioNTech, financed with German public money;
Moderna received 2.5 billion dollars in aid from the United States government ;
AstraZeneca benefited from a British government-funded laboratory at Oxford Public University to generate a free-access, patent-free vaccine with guaranteed low prices;
Various Russian and Chinese public institutes began to develop their own vaccines, especially Sputnik V of the Gamaleya Institute.
The division of procedures is clear: pharmaceutical companies have been characterized by benefiting from state / public funds and infrastructures for the benefit of private profit, while countries antagonistic to this business model sovereignly develop their vaccines with the intention of offering them in an accessible way the poorest countries on the planet.
Indeed, US efforts to dissuade countries from acquiring Sputnik V, while not entirely successful, have crystallized into a smear propaganda campaign wherever the Russian vaccine is distributed.
So this rise of the health corporations has been premeditated and sponsored even by the government of the United States, which, as many of us know, pressured the government of Brazil not to sign any contract with Russia to acquire Sputnik V because it is a kind of "malicious influence".
The fight for the covid vaccine market has a high economic impact, if we take into account recent statements by President Vladimir Putin , suggesting that the West has wanted to defame the scientific efforts of Russia because it is estimated that this market will reach 100 billion dollars. To get an idea of how gigantic those numbers, Russia's income from the sale of oil and its derivatives barely reaches those 100 billion dollars.
It is notable that the United States primarily promotes the Pfizer vaccine, but Moderna and AstraZeneca also have media and political support. Although not for long for the latter.
ASTRAZENECA AGAIN IN THE EYE OF THE HURRICANE
There are already several countries in Europe and other parts of the world where the use of the vaccine created by Oxford / AstraZeneca has been suspended . Although there are still no conclusive results from studies in these countries that determine the direct relationship between the vaccine and blood clots that have been found among those vaccinated, the situation is still tense, generating a drama that jeopardizes the prestige of this pharmaceutical, one of the biggest beneficiaries of public money.
Indian economist Jayati Ghosh recounts how the AstraZeneca vaccine was developed:
Doesn't everything Ghosh related sound more like fraud? Is it that hard to admit?The vaccine was developed entirely by a publicly funded laboratory at the University of Oxford. The original distribution model was for an open license platform, designed to make the vaccine freely available to any manufacturer. However, the Gates Foundation, which was influential because it had donated $ 750 million to Oxford for vaccine development, persuaded the university to completely change course and sign “an exclusive vaccination agreement with AstraZeneca that granted the giant pharmacist exclusive rights and no guarantee of low prices. "( Jay Hancock 2020 )
Oxford and AstraZeneca promised not to make a profit from the sale of the vaccine, but the details were left unclear. While Oxford will not receive royalties during the pandemic, it could subsequently benefit from patents, including those of Vaccitech, a for-profit spin-off.
Meanwhile, AstraZeneca is charging differential prices for its vaccines shipped to different countries, with some poorer countries paying higher fees. The European Union pays $ 3.50 per dose, while Bangladesh pays $ 4 and South Africa up to $ 5.25 ( Politico, 2021 ).
This price variation is not limited to AstraZeneca injection. Due to competition over doses and opaque contracts, the reported price range for vaccines is wide: from $ 2.19 to as much as $ 44 per dose, as of March 1. ( UNICEF, Covid Control Panel ).
Although the use of the vaccine in question is being suspended in the most important countries of the European Union, such as Germany and France, it has nothing to do with the business model imposed on the current global health context. Apparently there is nothing to criticize or transform there, according to those governments.
And yet it is curious that fraud has been a constant in AstraZeneca , not only during these pandemic months in which this company has been immersed in scandals of corrupt transparency in the contracts signed with the European Commission and on the delay and the amount of the doses agreed with each country, also in other periods of history, the Anglo-Swiss pharmaceutical company has been prosecuted in US and European courts for crimes more or less related to what has been outlined.
A brief search on the web reveals that in 2003 , 2010 , 2014 , 2018 and 2020 the AstraZeneca company has had to pay hundreds of millions of dollars for fraud cases in which its representatives have successively had to accept the guilt of the causes or have been found guilty in a procedural trial.
So it would not be the first time that the curriculum of this company has been tainted by public opinion, however that does not discourage the most conspicuous promoters of neoliberalism. On the contrary, impunity for these pharmaceutical companies prevails as a religious dogma and they will continue to undermine the interests of the global poor population with an eye on the lucrative drama that is injecting a market as large as the pandemic tragedy we are experiencing.
https://misionverdad.com/globalistan/el ... o-al-mundo
Google Translator
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis
Western Media Blitz Aimed at Russia’s Sputnik V Vaccine May Already Be Costing Lives
March 17, 2021
By Alan Macleod – Mar 15, 2021
People are already needlessly suffering as a result of renewed great power competition as a recent DHHS report reveals that the first deaths in the second Cold War may have already occurred.
Washington – A new report from the Department of Health and Human Services (DHHS) boasts that, throughout 2020, it worked with other U.S. government agencies to combat the “malign influence” of Russia, Cuba and Venezuela in the Americas. The two examples it cites are “persuading Brazil to reject the Russian COVID-19 vaccine” and pushing Panama to turn down Cuba’s offer to send doctors to fight the virus.
Partially as a result of refusing aid and following former president Trump’s every order, Brazil is beset by a rampaging virus, having lost over 278,000 people to COVID-19, behind only the United States in total deaths. Brasil Wire’s John McEvoy, who first reported on the news, saidU.S. actions had “likely kill[ed] thousands of Brazilians.”
Meanwhile, Panama’s outbreak is, per capita, even worse than Brazil’s, with the tiny nation having already lost 6,000 citizens to the virus.
The world’s most trusted vaccine
The Russian state-funded Sputnik V vaccine is one of the only options for the Global South, as rich, developed countries have hoarded other vaccines, ordering far more doses than would be necessary to treat their entire populations. At the same time, they have struck down attempts by poor nations to waive intellectual property concerns and produce the vaccine themselves — a move condemned by medical organizations like Medecins Sans Frontieres. This means that the Russian, Chinese, or a potential Cuban vaccine currently in the final testing stages are their only hope.
Sputnik V has also been subject to an intense Western propaganda campaign aimed at defaming it. In January, Twitter was even forced to suspend Sputnik’s official account after a hack was detected emanating from Virginia. “Now who in Virginia might want to sabotage a global health initiative by one of Washington’s “official enemies?” wrote former MintPresscontributor Morgan Artyukhina, strongly implying she believed one of the many three-letter agencies headquartered in the state was behind the hack.
Despite the defamation campaign, Russia is actually the most trusted vaccine manufacturer worldwide, according to a study of 11 countries conducted by British pollster YouGov. Over a billion doses have already been ordered globally, and a number of European Union members, including Hungary, Czechia and Slovakia, have broken ranks and unilaterally began administering the shot to their populations. An alarmed EU has tried to put a stop to it, urging caution. However, their words have proven ineffective, as the 27-nation bloc’s vaccine rollout has been distinctly lackluster.
Blood clots and blocked shots
Adding to Europe’s woes are the increased worries about the Oxford-AstraZeneca vaccine, with a great many European countries, including Ireland, Austria, Denmark, Bulgaria, Norway and Romania suspending its use. This is due to a potential link to blood clots reported in multiple nations.
The first reports of a potential link to clotting came from Austria. Then a number of Norwegians experienced similar problems, with one person dying. The Italian region of Piedmont also temporarily suspended its vaccination campaign to investigate whether the death of a local teacher had any connection to the jab.
“We can’t allow any doubts about the vaccine,” Dutch Health Minister Hugo de Jonge said, explaining his government’s decision to do the same. “We have to make sure everything is right, so it is wise to pause for now.”
Western media have been extremely cautious in reporting on concerns. In its article yesterday detailing the cavalcade of countries suspending its use, The Guardian included no less than seven separate rebuttals to the idea that the Oxford-AstraZeneca vaccine was dangerous.
Considering the gravity of the situation — a global pandemic that is raging out of control across five continents, already killing over 2.66 million people — this is a pertinent decision, especially as there is already a considerable lack of will among many populations to receive the vaccine.
Blood clots are a relatively common occurrence. Of the millions of people who have already been inoculated with the Oxford-AstraZeneca offering, there have been just 30 reports of blood clots, and only one fatality. One would expect a higher rate among a random sample of the population. It is therefore vastly more dangerous to be exposed to COVID-19 than risk any as yet unproven blood clot from the British vaccine.
The World Health Organization today reconfirmed its faith in Oxford-AstraZeneca. “There is no evidence that the incidents are caused by the vaccine and it is important that vaccination campaigns continue so that we can save lives and stem severe disease from the virus,” they stated.
“Reckless and unethical”
The Guardian’s sobriety is in complete contrast to how it has portrayed Sputnik V, describing it as “controversial,” its development “reckless and unethical,” claiming there was a “rising chorus of concern” from experts about its safety, and generally framing it as unconvincing and suspicious. This naysaying only appeared to change after it was announced that Sputnik V might be combined with Oxford-AstraZeneca to increase effectiveness. Last month, the Lancet, the most prestigious medical journal in the world, came out to fully endorse Russia’s vaccine offering as both safe and effective.
NY Times Sinopharm bias
Meanwhile, much of Western reporting on the Chinese Sinopharm vaccine has been beyond irresponsible. Reuters, for example, published an article entitled “Peru volunteer in Sinopharm vaccine trial dies of COVID-19 pneumonia, university says.” Yet later the same article reveals that she had, in fact, not even received a vaccine, but was part of a control group receiving a placebo. Meanwhile, The New York Times ran a story with the headline “Brazil resumes Chinese vaccine trial after a brief suspension following the death of a volunteer.” The person in question committed suicide, as the article notes. However, the majority of news consumers do not read past the headline, meaning that both these examples sow false doubt about the Chinese vaccine’s effectiveness. This, or the desire to generate traffic with clickbait, are the two most likely explanations for such misleading journalism.
It is a similar story on social media. Twitter’s editorial team put up a message today on its homepage noting that there is no causal link between Oxford-AstraZeneca and blood clots. It has also banned users who spread COVID-19 conspiracy theories about Western vaccines. Yet defaming those from America’s official enemies is commonplace on its platform. “Since Russia so flagrantly cheated in sport’s doping over decades, why would anyone trust data coming out of Russia for their Sputnik vaccine?” Bill Browder, CEO of Hermitage Capital tweeted last week to his audience of over a quarter million people.
The Guardian warned that the mass uptake of Russian and Chinese vaccines across the Global South meant that the West was “falling behind in the race for influence.” Considering that the U.S. is offering little except pressure not to take up Russia, China or Cuba’s offers, they are probably correct. Corporate media’s worry over so-called “vaccine diplomacy” hints at a broader reason for the negative coverage of the Russian and Chinese offerings.
The second Cold War
It is little secret that we are entering a second Cold War with both Russia and China. War planners and policymakers have, for years, been discussing how to attack those nations militarily, economically and through propaganda.
In recent months, the U.S. has sent warships and bombers to the South China Sea, testing Chinese coastal defenses. In July, American destroyer the U.S.S. Rafael Peralta sailed just 41 nautical miles from the coastal megacity of Shanghai. President Trump also attempted to impede China’s economic rise, placing sanctions upon the country and attempting to stop the spread of Huawei’s global 5G network. Meanwhile, some U.S. war planners are advocating a wholescale psychological war against China. The Pentagon’s budget request for 2021 makes clear that they envisage a shift away from the Middle East and towards Russia and China as their new focus.
The U.S. public has already been convinced, by and large. After years of negative publicity, Americans’ opinions of those two nations have slumped to below 1980s levels, with only 22% and 20% of the public holding positive opinions about Russia or China, respectively.
Virtually all the victims of the first Cold War were in the Global South, in countries such as Vietnam, Cambodia or Guatemala. People are already needlessly suffering as a result of renewed great power competition. What this latest DHHS report reveals is that the first deaths in the second Cold War have already occurred.
https://orinocotribune.com/western-medi ... ing-lives/
I'd bet a dollar that there is a US rat behind the A/Z blood clot thing . Seems like most everybody know that it ain't a 'thing' but the combination of propaganda, engineered ignorance and tech mitigate against the dismissal that logic demands.
I was torn initially about Sputnik: the basis upon Soviet science vs the ham-handed capitalism of the Russian oligarchs, but 'proof of the pudding'....Leave it to the polished Western oligarchs to show how it's really done.
PS- Please please please no more photos of needles/vaccine
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis

Iranian scientist with samples of the vaccine made in the Islamic Republic (Photo: Abedin Taherkenareh / EPA-EFE)
Eder Peña
20 Mar 2021 , 11:50 am .
The race for vaccines has made the global pandemic continue to reveal the true rules of the world political game. Disputes over territories, resources and even the cultural hegemony that the West has sought to impose on the rest of the world through its globalizing locomotive have been laid bare today.
There is a list of countries that Western countries consider threats for not giving in in such disputes or privileging the "market" (their transnationals) above all else. There have been various established conflicts and unconventional warfare methods to achieve changes in their regimes that escalate as they fail.
THE GLOBAL RACE FOR VACCINES, PARTY OF PRIVILEGES
According to the World Health Organization (WHO), as of February 18, 2021, there were at least seven different vaccines that countries were starting to administer on three platforms, prioritizing vulnerable people in all cases. Additionally, there are more than 200 experimental vaccines in development, of which more than 60 are in the clinical phase.
According to a report by the Intelligence Unit of The Economist , the United Kingdom, the United States, Israel, Hong Kong, Singapore and the European Union (EU) will be the only territories with their entire adult population vaccinated before the end of 2021.
On the other hand, high-income nations such as Canada, Japan, and Australia, and middle-income countries such as Mexico, Chile, Argentina, Brazil, Russia, and South Africa will be able to reach the goal by mid-2022. By contrast, nearly all nations in Africa and the Northern Triangle of Central America will not see that goal met until the end of 2023, a year and a half after the first countries reached the goal.
The Economist report takes into account aspects such as purchase contracts, production, vaccine availability, population size and the vaccination logistics deployed. According to data compiled by the Duke Global Health Innovation Center at Duke University, the countries or entities that had the highest number of doses ordered by number of inhabitants were the following:
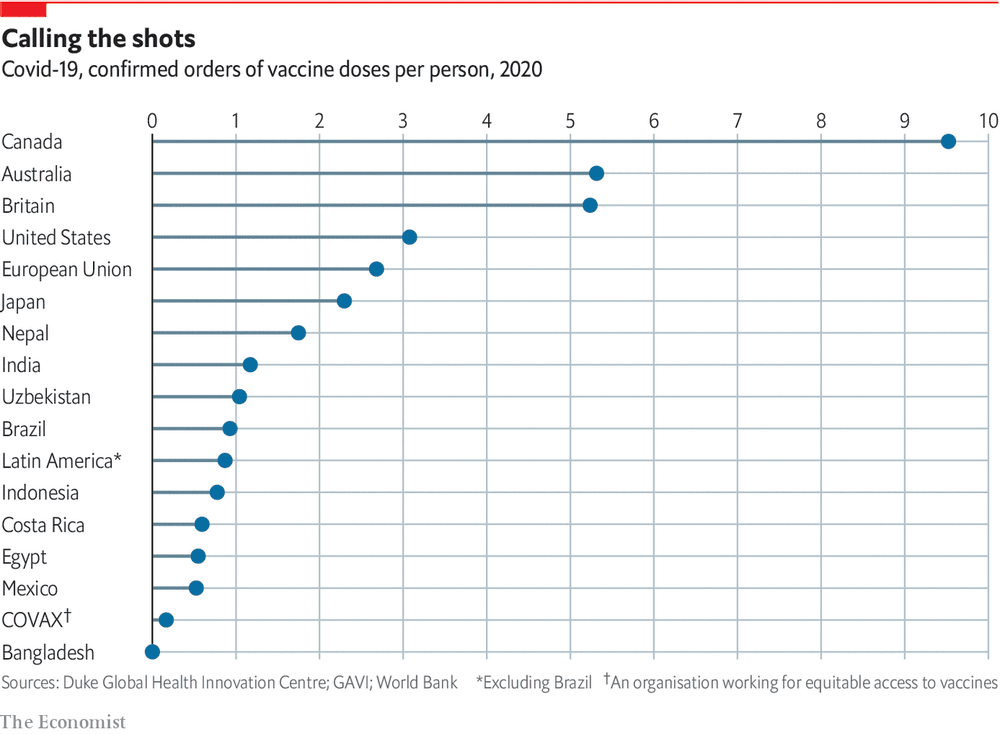
Confirmed orders for covid-19 vaccine doses per person according to countries or entities (Photo: The Economist)
As seen in the list above, many rich countries like Canada, home to 36 million people, have enough doses to vaccinate 169 million, almost five times more than their total population. Japan has a population similar in size to Mexico, but has guaranteed the purchase of 314 million doses, which will be able to cover its adult population without difficulty, without having to resort to additional purchases.
Not only does it happen that half of the vaccine inventories are reserved for 15% of the world's population, nor that apartheid and siege mechanisms have been developed , but rather that it seeks to implement control mechanisms such as, for example, the required digital passport. for people entering the EU.
Even though it is not mandatory to be vaccinated, the EU presented at the beginning of this month a proposal to introduce its "vaccine passport" to help free movement within the block, but it will only be valid with vaccines approved by the Agency European Medicines Agency (EMA), i.e. Pfizer / BioNtech, AstraZeneca, Moderna and Johnson & Johnson.
The countries that the United States and its satellite countries have identified as "axis of evil" have initiated actions both to develop their own vaccines and to maintain high levels of cooperation since the pandemic began. This is how, one year after the worst health emergency of the current century, they have sought to circumvent the interested management of that imperial bloc that maintains sanctions on more than a quarter of the people on Earth .
RUSSIA TOOK THE FIRST STEP OF MANY
It was the first country to register a coronavirus vaccine, but there are more than 20 in the testing and development phase, all different from each other. Even when developed by the same institutions, each has its own "nuances".
In phase 3 of clinical trials are Sputnik V, the first registered in the world, and the Siberian vaccine called EpiVacCorona.
EpiVacCorona is being investigated at the Vector Siberian science center, founded in 1974 primarily as a laboratory dedicated to military research. It is a vaccine based on viral proteins and peptides, which means that these proteins are not produced in the patient's cells, but are injected directly into the body together with sensitizing substances to which the immune system reacts.
On August 12, the third stage of the study began, which is considered the most important, since all the unlikely side effects can be identified in a large sample. More than 2,000 people from Russia, Saudi Arabia, Brazil, Mexico, the United Arab Emirates and other countries participated. The vaccine was registered in Russia in October.
Sputnik V, which was developed by the Gamaleya Institute of Epidemiology and Microbiology of the Russian Ministry of Health, in a joint research project with the 48th Central Research Institute of the Russian Ministry of Defense, has three analogues in the world: the Oxford vaccine- AstraZeneca , that of the Chinese company CanSino and that of Johnson & Johnson. They are all developing an adenoviral vaccine, not with two, but with one vector. This vaccine is launched in two stages: first a vector, then the second.
The Lancet, one of the oldest and most respected medical journals in the world, has published the interim results of a phase III clinical trial of Sputnik V, confirming the high efficacy and safety of the vaccine. The head of Russia's Direct Investment Fund, Kirill Dmitriev, reported that it is one of three vaccines worldwide that is more than 90% effective and outperforms the other two in terms of safety and ease of transport due to the storage requirements of +2 to + 8ºC and a more affordable price. "
CHINA, VACCINES WITH LOW LEVELS OF SIDE EFFECTS
On Monday 15, China authorized the emergency use of a new vaccine developed by its Center for Disease Control (CDC, for its acronym in English), it consists of protein subunits, according to a statement published by the Institute of Microbiology of the Chinese Academy of Sciences. The drug was jointly developed by Anhui Zhifei Longcom Biopharmaceutical Co. Ltd. and the Chinese Academy of Sciences and was approved for use in Uzbekistan on March 1.
The other three main Chinese laboratories that have developed vaccines against COVID-19 are Sinopharm, CanSino and Sinovac. Sinopharm already has two vaccines that have been developed, one from a coronavirus obtained from a patient in Beijing and another from a patient in Wuhan.
Both types of viruses were cultivated and, from them, two vaccines were obtained that were developed following the traditional method of inactivating them with chemical substances so that the viruses lose their ability to cause infection, but maintain their ability to awaken the formation of neutralizing antibodies by the defense system.
Results published in The Lancet in January 2021 show that the vaccine developed in Beijing, already approved in China, is safe and capable of stimulating the production of neutralizing antibodies. It requires two doses and its efficacy was estimated at 79.34%, so on December 31 it was approved for emergency use by the Chinese regulatory entity.
Both are being tested in phase 3, mostly in 10 countries in Latin America and the Middle East, and a great advantage for their use in medium to low-income countries is that they do not require freezing for storage and transport.
On the other hand, CanSino, in association with the Institute of Biology of the Chinese Academy of Military Medical Sciences, has developed a one-dose vaccine that is based on a vector, a cold virus called Ad5. The Lancet and its phase 2 studies, published in July 2020, showed that the vaccine produced a strong immune response, and in an unprecedented move, the Chinese military approved its use in June as a "particularly necessary drug." CanSino began its phase 3 studies in several countries in August, including Pakistan, Russia, Mexico and Chile.
While Sinovac, a private Chinese company, developed a vaccine called CoronaVac that is based on an inactivated virus like Sinopharm's. Their phase 1-2 studies were published in The Lancet in November 2020 and they were shown to have comparatively modest neutralizing antibody production in 743 volunteers, with no serious adverse effects.
The efficacy of CoronaVac has been the subject of uncertainty, in a phase 3 study developed last January in Brazil, it reached an average efficacy of 50.38%, highlighting that it could prevent almost 78% of mild cases and 100% of cases. moderate and severe.
With the exception of Sinovac, all have high levels of efficacy and have shown low levels of side effects. Due to their storage in common refrigerators, they have a great advantage for use in low and middle income countries but, according to experts, they will be one of the most expensive on the market.
CUBA, A PIONEER IN LATIN AMERICA AND THE CARIBBEAN
The Caribbean island is simultaneously developing five vaccine candidates: Soberana 01, Soberana 02. Soberana Plus (or Soberana 1A), Mambisa and Abdala, last February its government announced that tourists who arrive will be offered the opportunity to get vaccinated and if so they wish.
Vicente Vérez, director of the medical research center of the Finlay Institute in Havana, announced his intention to produce 100 million doses of the Sovereign 02 vaccine this year and inoculate the entire Cuban population of 11.3 million people. More recently, the President of the Republic, Miguel Díaz-Canel Bermúdez, highlighted that two provinces would enter phase 3 of the clinical trials of the vaccine candidate Abdala, which will be approved by the Center for State Control of Medicines, Equipment and Medical Devices from Cuba (Cecmed).
The BioCubaFarma business group also announced that Abdala's production system, made up of the Center for Genetic Engineering and Biotechnology (CIGB) and the company Laboratorios AICA, has guaranteed the necessary doses for this phase, which would include 42 thousand people.
Soberana 02 is the first Latin American project in the fight against covid-19 to reach phase 3, the application of the first dose of the vaccine and the placebo has already begun in 44 thousand 10 volunteers from eight municipalities in the province of Havana . A second injection will be applied after 28 days and in a number of cases a third booster dose will be added with another Cuban vaccine candidate, Soberana 01A or Soberana Plus, which will be intended for people convalescing from the disease.
The president of the state group BioCubaFarma, Eduardo Martínez, told the official newspaper Granma that it is expected to have "by August at the latest" the millions of doses of the vaccine it needs to immunize "its entire" population, and then continue to manufacture them for help "friendly countries".
I RÁN ADVANCES DECISIVELY WITH SANCTIONED VACCINE
The Iranian authorities have repeatedly denounced the negative impact of "economic and medical terrorism" in Washington and the restrictions that make it difficult to import medicines, equipment and basic necessities, calling them "crimes against humanity".
Last February they began clinical trials in humans of their second vaccine candidate against covid-19 of at least eight, called Razi CoV-Pars, which is both injectable and intranasal and is based on recombinant covid-19 proteins.
The first, COVIRAN Barekat, has entered its clinical trial phases 2 and 3 , while Razi COV-Pars is a recombinant protein S or spike of the virus, type messenger RNA vaccine. It will be administered by injection and inhalation, it was developed by one of the oldest and most reputable research centers in the country, the Razi Vaccine and Serum Research Institute.

A member of the medical staff of the Imam Khomeini Hospital receives a dose of the Sputnik V vaccine in Tehran on February 9 (Photo: Reuters)
Last February, Minu Mohrez, member of the National Committee for the Management and Fight against Coronavirus declared that COVIRAN Barekat is as effective in combating the British variant of the new coronavirus as the original virus (90% in humans) and, until now , there have been no side effects from its inoculation.
At the end of last year, the Iranian authorities stated that the country has the capacity to produce about 1.5 million doses of COVIRAN Barekat per month, a figure that will rise to 12 million doses per month during the next semester. Its developers were sanctioned by the United States immediately after the order of the Leader of the Islamic Revolution of Iran, Ayatollah Seyed Ali Khamenei, prohibiting the purchase of American vaccines, calling them unreliable.
Last Tuesday 16 , Fakhra was presented , the third to enter the clinical trial phase in the country, by the Defense Research and Innovation Organization of that country, which began in December 2019 and has successfully passed the first phase of trials. clinicians.
It should be noted that this vaccine pays tribute to the Iranian scientist assassinated last November 2020, Mohsen Fajrizadeh , who also led the vaccine project until his death. Iranian authorities and health officials have said that within three months Iran will become the leading manufacturer of coronavirus vaccines in the Middle East.
PANDEMIC DIPLOMACY WESTERN VERSION: DO NOT DO OR LET DO
Accusations of using vaccines as a geopolitical weapon or of "vaccine diplomacy" have not stopped since they began to be developed but have intensified with distribution. In this regard, the global press has divided the world into two camps: one represented by the countries inoculated with Chinese and Russian vaccines and the other with American and European vaccines.
The United States and its allies, while bragging about their own vaccines, question the safety and efficacy of Chinese vaccines and label China and Russia as the pioneers of the global campaign of "vaccine diplomacy."
For their part, the governments of China, Cuba, Iran, Nicaragua, North Korea, Russia, Syria and Venezuela, all under United States sanctions, sent a joint statement to the United Nations Secretary General, the United Nations High Commissioner United for Human Rights and the Director General of the World Health Organization calling for the end of the US unilateral economic blockade, as it were, "illegally and flagrantly violates international law and the charter of the United Nations."
The truth is that the results show that the state investigation on covid-19 vaccines in Russia, China, Iran and Cuba beat the American " public-private partnership ", the Russian government announced last August that it had registered the first covid vaccine. 19 of the world, called Sputnik V, at the same time that Trump ironized about the vaccine and about the severity of the pandemic.
In response, as usual, the United States Department of Commerce imposed sanctions on Russia's 48th Central Research Institute for being associated with Russian chemical and biological weapons programs, allegedly, while its program, called "Operation Warp Speed", eliminated Billions of dollars in taxes on Big Pharma.
At the beginning of March, AFP reported that Christa Wirthumer-Hoche, president of the EMA board of directors, "advised against" the member countries of the European Union (EU) to urgently authorize Sputnik V, alleging insufficient data on the vaccinated people, as he would have declared in an interview with the Austrian television channel ORF, adding that "it is a bit like Russian roulette."
The United States and the EU have stigmatized China and Russia since last August, however Hungary, Serbia, Czech Republic or Slovakia, EU member countries, have opted for Russian or Chinese vaccines because vaccination campaigns have not yet started in their territories after almost two months, this due to the slow implementation by Brussels. As a consequence there have been internal clashes in their governments and furious statements from the cartelized press of those ex-socialist countries.
The failures in the vaccination campaigns in full escalation of infections have once again demonstrated the place that Eastern European countries occupy within the EU (Photo: Diario Milenio)
Other EU members such as Bulgaria, Croatia, Estonia, Latvia and Romania are awaiting EMA approval for Sputnik V; Montenegro, Bosnia and Herzegovina, North Macedonia and Kosovo, have not yet started vaccination campaigns in full escalation of infections, without a specific schedule for the delivery of COVAX mechanism vaccines, without approval of the use of Chinese or Russian vaccines, or the EU procurement plan. Lithuania and Poland have ruled out both vaccines.
On this side of the Atlantic: the United States Department of Health and Human Services confirmed that its international team, the Office of Global Affairs (OGA), "used diplomatic relations in the Americas region to mitigate the efforts of states, including Cuba, Venezuela and Russia, who are working to increase their influence in the region to the detriment of the security of the United States. "
HIGH LEVELS OF COOPERATION WITHIN THE "AXIS OF EVIL"
Faced with the war implanted against countries not aligned with the unipolar vision imposed by the United States' war party, actions based on multipolarity have been carried out, some examples:
Since the beginning of the pandemic, Russia and China have maintained high-level exchanges and mutual political trust and pragmatic cooperation have been deepened in various areas, particularly in the sharing of experiences in prevention, control and treatment, and they have also sought to promote joint scientific research, address common threats and challenges, and maintain global public health security.
The announcement of the inoculation of the Sovereign 02 vaccine from next April in Iran made last February due to the joint development of the drug between Cuba and the Islamic Republic. Both countries reached an agreement in early January to cooperate in supplementing the clinical evidence of the Cuban vaccine candidate.
While Iranian vaccines are being prepared, the country has received two first shipments of Sputnik V and 250,000 doses of Chinese vaccines for the inoculation of health personnel and the most vulnerable. In addition, Tehran and Moscow have agreed to transfer the vaccine technology to Iran.
With the 17 tons of materials and medical supplies received from China, which included a batch of 500 thousand doses of the Sinopharm vaccine, "more than 550 tons in total are reached, if we add the cooperation agreements and purchases that Venezuela has made with other countries and with multilateral organizations, "declared Venezuelan Foreign Minister Jorge Arreaza.

Cooperation with China has allowed both Venezuela and other countries that suffer from the "sanctions" of the United States and its allies, have inputs to face the global pandemic and investigate how to overcome it (Photo: File)
China has donated materials to more than 150 countries, regions and international organizations around the world in the midst of the global pandemic, while Cuba has sent more than 30 medical brigades from the Henry Reeve International Contingent, to support the fight against the disease. The company Changchun Heber Biological Technology Co. Ltd (ChangHeber), manufactures more than 180 biotechnological products, among which is Interferon Alpha-2B, used against SARS-CoV-2.
The China-Latin America Bulletin published annually by the Center for Global Development Policies of Boston University recorded that Venezuela received practically half of the medical aid that China delivered to Latin America since the beginning of the pandemic, of the 215 million dollars in medical aid that it gave to the region, more than 100 million went to Venezuela.
https://misionverdad.com/investigacione ... poyo-mutuo
Google Translator
Covid is a hard, remorseless lesson of the inferiority of Western capital in meeting human need. When even the paleo-capitalist regime in Russia is beating you in 'vaccine-diplomacy' you're pretty sorry.
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis
Britain’s Covid-19 care home cull
Linocut by Ramona Sharples, 2021
'We did everything we could have done and we will carry on doing everything we can.' This is how Boris Johnson characterised government policy on 26th January 2021, as Britain headed past the 100,000-death mark, with disabled people accounting for 60%. Bear this quote in mind as you read through this account of government actions towards care homes over the past year, and how care home residents account for between a third and 40% of deaths, yet they represent just 0.65% of the population. And that’s at least 10% of care home population culled, without even taking into account indirect causes of death; a study by the University of Manchester in November estimated that care home death toll was undercounted by 10,000. Journalist Julia Hartley-Brewer – citing official NHS England figures published on 19th November that 96% of Covid-19 deaths had ‘pre-existing health conditions’ and 92% were aged over 60 – concluded that the pandemic response has been overblown. After all, who cares about over-60s or pre-existing conditions? This is supposedly Britain’s ‘Greatest Generation’, yet more have been killed by Covid-19 than by the Blitz (which took approximately 32,000 lives).
Why is the British ruling class, exemplified by the likes of Julia Hartley-Brewer, so callous about the lives of our grandmas and grandads? Money, essentially. Those with non-standard bodies (and minds) slow down the production process and in various ways are a drain on profit for capitalists. They’re ‘unproductive’ as far as businesses are concerned. The ‘unproductive’ include the elderly and the disabled, and Britain’s ageing population has been a source of concern for its ruling class for a long time. The Office for National Statistics predicted that 25% of Britain’s population will be over 65 by 2066, and they already outnumber under 16s; a Times article from 2018 was headlined: ‘An ageing population is posing problems that Britain cannot ignore’; and in 2017, the Conservative Party tweeted, ‘There will be two million more people over 75 in the next 10 years – we to have a plan to deal with that challenge.’ Covid-19 presented the government with a convenient solution.
The government had already been killing the elderly for years through pension cuts, depriving them of heating funding (during the winter, the cold kills an elderly person every 5 minutes or so), while the disabled have suffered attacks (over 17,000 have died while waiting for benefits) through the bedroom tax, benefit sanctions, and austerity cuts to council services. The NHS has been decimated and left unfit for purpose and the disabled have been increasingly segregated into underfunded care homes and deprived of accessible housing. Segregation has intensified by allowing landlords to operate ‘no benefits’ prerequisites for tenants, reminiscent of ‘no blacks, no dogs, no Irish’, and care has been outsourced to (often untrained) volunteers as much as possible.
Care homes are, you’ll be shocked to discover, actually homes, not hospitals, and care staff are not necessarily qualified to nursing level – nor do they have adequate stocks of PPE at the ready. Care homes are places where people live; they have the right not to be exposed unnecessarily to a lethal disease. To give an insight into the horror of the situation: approximately 350 non-Covid patients died of thirst in care homes and hospitals during the first lockdown, let alone anything else. The British Medical Journal recent editorial characterised governments such as Britain as committing ‘social murder’ in their response to the pandemic. Friedrich Engels first described this in 1845:
‘When one individual inflicts bodily injury upon another such that death results, we call the deed manslaughter; when the assailant knew in advance that the injury would be fatal, we call his deed murder. But when society places hundreds of proletarians in such a position that they inevitably meet a too early and an unnatural death, one which is quite as much a death by violence as that by the sword or bullet; when it deprives thousands of the necessaries of life, places them under conditions in which they cannot live — forces them, through the strong arm of the law, to remain in such conditions until that death ensues which is the inevitable consequence — knows that these thousands of victims must perish, and yet permits these conditions to remain, its deed is murder just as surely as the deed of the single individual; disguised, malicious murder, murder against which none can defend himself, which does not seem what it is, because no man sees the murderer, because the death of the victim seems a natural one, since the offence is more one of omission than of commission. But murder it remains.’
The government didn’t send hitmen in with guns to massacre care home residents, but that doesn’t mean it isn’t a form of murder. Here’s how it happened.
Discharge and legislation
On the 27th of May, Boris Johnson – famed around the world for his honesty – declared ‘it’s just not true that there was some concerted effort to move people out of NHS beds into care homes.’ The NHS reserved 1800 beds in care homes right at the start of the pandemic and proceeded to discharge 25,000 patients between 17th March and 15th of April in England (plus about a thousand each in Wales and Scotland). Most weren’t even tested and, of those that were, patients who tested positive were discharged anyway (7 in Hull, 20 in Bristol and so on, 20% of care homes admitted patients with Covid-19 positive tests).
The government published guidance on 2nd April, titled ‘Admission and Care of Patients during Covid-19’, which stated:
‘the care sector also plays a vital role in accepting patients as they are discharged from hospital… Some of these patients may have Covid-19, whether symptomatic or asymptomatic… Hospitals around the country need as many beds as possible to support and treat an increasing number of Covid-19 cases. This means the NHS will seek to discharge more patients into care homes for the recovery period’.
No concerted effort, indeed. A Sky News survey of care homes found 70% of care homes felt pressured to take Covid-19 patients.
From April 15th, care homes received the formal ability to demand a test and reject Covid-19 patients, however, local councils replied by threatening to withhold pandemic funding unless they took patients in. Leading voices in the care sector also revealed that the £600m fund from the government actually prevented them spending the money on PPE for staff. Guidance was updated on September 16th reiterating that care homes should still be prepared to take Covid-19 positive patients from hospitals.
While the door was forced open to care homes, the door to hospitals was slammed shut. NHS hospitals were often operating a ‘no admissions’ policy for care home residents. The reason given for all of this was to prevent the NHS reaching capacity. Yet the Nightingale hospitals created specifically to deal with Covid-19 treated barely a trickle of patients, and then were largely kept ‘in hibernation’. The Nightingale hospital in London Docklands was arranged to have 4,000 beds, opening in early April, but the 7 hospitals across the entirety of England admitted hardly any patients at all (about 50 in London and approximately 100 in Manchester), and only briefly before they were put into ‘hibernation’ with potential capacity of several thousand beds and costing tens of millions in maintenance. Moreover, the NHS did not near capacity at any point; Alex Thomsen of Channel 4 news tweeted on 14th April: ‘Govt policy is to push recovering Covid hospital patients into care homes because NHS needs beds. Odd since no major hospital seems to be full and vast Nightingale field hospitals lie all but empty’.
Further to this, the fact that the government felt it necessary to grant legal immunity to health services and local authorities providing care for disabled people with the 2020 Coronavirus Act on 25th March and essentially suspend the legal duty to meet the needs of the disabled, could be considered a smoking gun. When discussing these facts with various people I tend to get the response: if this were true, there’d be a huge outcry. Well, let’s hear it from the government’s own ministers and MPs. Ros Altmann, former government minister, said care home residents ‘are being abandoned like lambs to the slaughter.’ She told Today:
‘They are left without protective equipment, they can’t find it, or testing even if they request it, it’s not always given to them. They haven’t got the staff they need … and they feel that the NHS has kind of left them in the lurch. GPs are not coming into the care homes in the way that they used to and some are finding if people need to be hospitalised either that tends to be very difficult or if people are sent to hospital they are sent back very quickly and there are no tests so they don’t know if these people are infecting others in their care homes.’
Tory MP Geoffrey Clifton-Brown characterised government approach to care homes as a ‘pretty reckless policy.’ Even Jeremy Hunt attacked his own government and a cross-party public accounts committee reported on 29th July that the Department of Health and Social Care (DHSC) had continued with the policy ‘even once it was clear there was an emerging problem’, and the chair (Meg Hillier MP), said ‘our care homes were effectively thrown to the wolves, and the virus has ravaged some of them.’
In response to criticism, Health Secretary Matt Hancock simply stated that it was not illegal. Boris Johnson shifted blame onto the care homes themselves: ‘We discovered too many care homes didn't really follow the procedures in the way that they could have.’ However, they followed the procedure of accepting Covid-19 positive patients as a fait-accompli – this is what caused the death toll. Labour provided zero opposition and their Five Point Plan in September didn’t even mention the seeding of the virus among those most vulnerable to it.
Floating cover staff, inspectors, and testing
The virus was further spread by allowing floating cover staff to move between different care homes, according to a study using genome tracking by Public Health England (PHE). Conducted from 11th to 13th April, results were known since – at the latest – the end of April, but weren’t circulated to care homes until weeks later. During this time at least 2,500 people died in English care homes. A report as far back as 2018 from flu pandemic planners warned ministers about controlling ‘cross-infection’ from such frontline temporary care workers.
A further document by PHE in 2019 regarding flu pandemic prep urged operators to avoid moving staff between homes and floors, yet the DHSC’s plan published on 16th April refrained from giving this same guidance which is so crucial in saving lives. In November The Telegraph reported that the government still hadn’t stopped agency workers from ‘roving’ across multiple sites, yet the spread of infection in care homes accounted for 82% of multiple outbreaks in the four weeks prior to the 8th of October, according to PHE.
In August the Care Quality Commission was repeatedly denied testing for its inspectors, a further risk of spread between 500 care homes planning to be inspected over a six-week period. The care sector trade union, GMB, predicted that inspectors would spread the virus ‘like wildfire’ through care homes: ‘we can’t comprehend why the government would deny inspectors access to testing.’ Technically, care staff have been eligible for tests since 28th April 2020, but the DHSC capped the daily amount of care home tests at 30,000 (both staff and residents). Tests were outright denied to people with learning disabilities and autism in care homes. Government guidance from the 15th April and updated on 14th May stated: 'you can only get tests if your care home looks after older people or people with dementia.' By the June 6th deadline for testing all care sector staff, the government had only managed about a third.
DNRs & frailty scale
At the beginning of the pandemic a ‘frailty index’ was created by the National Institute for Health and Care Excellence (NICE) to assess viability for critical care – those scoring above five on a scale of nine would be considered potentially disqualified from critical care. That included the ‘moderately frail’ – the patients who need help with complex tasks like financial management, transport, or heavy housework. NICE were soon forced to make U-turn on their advice for the NHS to deny disabled people treatment, but only after threats of legal action from disability groups. This index didn’t have a huge amount of time to do much damage, but is nevertheless another major indication of intent. The use of ‘Do not attempt resuscitation’ notices, on the other hand, functioned in a similar way, but were unable to be stopped in their tracks.
DNR notices waive the patient’s right to life. Typically these are signed by doctors in consultation with patients or failing that, their families, in situations where it’s in the best interests of the patient, in terms of minimising suffering, for them not to be resuscitated. One in ten care homes were told to place blanket DNRs on their residents or found that decision was taken by NHS staff without consultation with patients or their families, a report in August by Queen’s Nursing Institute found. Other patients were given DNRs as soon as they caught Covid-19. Some care homes delayed calling ambulances because of the DNRs. Residents 'felt pressured to agree to an advance Covid-19 care plan that stated they would stay at home without treatment if they contracted the virus.'
GPs across the country were writing to vulnerable patients advising them to fill out DNR forms in order to prioritise more able-bodied cases of Covid-19. One GP in Somerset recommended that autistic adults in care homes needed DNRs and another in Scarborough tried to apply it to an 11-year-old boy with cancer. Between July 2016 and December 2018, 19 hospital patients who died had ‘learning disabilities’ or ‘Down’s Syndrome’ given as the reason not to resuscitate. Turning Point, a learning disability care provider, stated that it had received an ‘unprecedented’ number of unlawful DNR orders for its patients. Hancock promised to ‘take action’ on wild use of DNRs, only after threat of a judicial review on 14th July. Yet, as late as October a press release by Amnesty International stated,
‘The horrifyingly widespread use of [Do not attempt cardiopulmonary resuscitation] orders for care home residents is one of the most deeply disturbing scandals of the pandemic. There’s no doubt that this was a violation of residents’ human rights and could have caused avoidable deaths… As we speak, countless do-not-resuscitate orders may remain in people’s files. Many of these people could fall ill in the coming months… It is also imperative that mechanisms are urgently put in place to ensure that there is full awareness across the health and social care sector that do-not-resuscitate orders must never be interpreted as meaning a person should not be transferred to hospital or receive other types of medical treatment.’
Furthermore it was found that around two thirds of people with underlying conditions (such as diabetes, high blood pressure, respiratory issues like asthma) were denied care during the pandemic.
It doesn’t matter to what extent this was premeditated and fully deliberate. Whether the government actively wanted to kill residents or simply didn’t consider them worthy of keeping alive is moot; the outcome is the same: social murder. A massacre, in fact. The government does have a motive, it had the means and it had the opportunity. They’ve tried to maintain plausible deniability, and this will be accepted by those who are in the habit of whitewashing Britain’s crimes and murderousness even in the face of overwhelming evidence. The crimes of Britain are legion and include, pointedly, use of germ warfare to commit mass murder and even genocide (using disease against Native Americans and First Nations in what is now the USA, Canada and Australia, and then between 1940-1979 tested biological weapons, including anthrax, on its own citizens in Britain, affecting the elderly in particular). The Conservative Party openly talked about the elderly and the disabled as posing a problem and a financial burden, before the government actively funnelled a lethal virus into care homes which house the very people most vulnerable to the disease. They deprived them of testing, protective equipment and other essential resources. They allowed floating cover staff and inspectors to exacerbate the spread, denied residents access to hospitals and forced DNRs on them. Case closed.
Pitchfork Cosmonaut writes on anti-imperialist current affairs, history, and pop culture, and you can find them on Twitter @pitchforkcosmo.
With special thanks to Prolekult, whose dedicated ongoing research of this issue has been fundamental to the writing of this piece. Make sure to watch their incredible documentary on this topic: Camps of Dependence.
https://www.ebb-magazine.com/essays/bri ... -home-cull
Linocut by Ramona Sharples, 2021
'We did everything we could have done and we will carry on doing everything we can.' This is how Boris Johnson characterised government policy on 26th January 2021, as Britain headed past the 100,000-death mark, with disabled people accounting for 60%. Bear this quote in mind as you read through this account of government actions towards care homes over the past year, and how care home residents account for between a third and 40% of deaths, yet they represent just 0.65% of the population. And that’s at least 10% of care home population culled, without even taking into account indirect causes of death; a study by the University of Manchester in November estimated that care home death toll was undercounted by 10,000. Journalist Julia Hartley-Brewer – citing official NHS England figures published on 19th November that 96% of Covid-19 deaths had ‘pre-existing health conditions’ and 92% were aged over 60 – concluded that the pandemic response has been overblown. After all, who cares about over-60s or pre-existing conditions? This is supposedly Britain’s ‘Greatest Generation’, yet more have been killed by Covid-19 than by the Blitz (which took approximately 32,000 lives).
Why is the British ruling class, exemplified by the likes of Julia Hartley-Brewer, so callous about the lives of our grandmas and grandads? Money, essentially. Those with non-standard bodies (and minds) slow down the production process and in various ways are a drain on profit for capitalists. They’re ‘unproductive’ as far as businesses are concerned. The ‘unproductive’ include the elderly and the disabled, and Britain’s ageing population has been a source of concern for its ruling class for a long time. The Office for National Statistics predicted that 25% of Britain’s population will be over 65 by 2066, and they already outnumber under 16s; a Times article from 2018 was headlined: ‘An ageing population is posing problems that Britain cannot ignore’; and in 2017, the Conservative Party tweeted, ‘There will be two million more people over 75 in the next 10 years – we to have a plan to deal with that challenge.’ Covid-19 presented the government with a convenient solution.
The government had already been killing the elderly for years through pension cuts, depriving them of heating funding (during the winter, the cold kills an elderly person every 5 minutes or so), while the disabled have suffered attacks (over 17,000 have died while waiting for benefits) through the bedroom tax, benefit sanctions, and austerity cuts to council services. The NHS has been decimated and left unfit for purpose and the disabled have been increasingly segregated into underfunded care homes and deprived of accessible housing. Segregation has intensified by allowing landlords to operate ‘no benefits’ prerequisites for tenants, reminiscent of ‘no blacks, no dogs, no Irish’, and care has been outsourced to (often untrained) volunteers as much as possible.
Care homes are, you’ll be shocked to discover, actually homes, not hospitals, and care staff are not necessarily qualified to nursing level – nor do they have adequate stocks of PPE at the ready. Care homes are places where people live; they have the right not to be exposed unnecessarily to a lethal disease. To give an insight into the horror of the situation: approximately 350 non-Covid patients died of thirst in care homes and hospitals during the first lockdown, let alone anything else. The British Medical Journal recent editorial characterised governments such as Britain as committing ‘social murder’ in their response to the pandemic. Friedrich Engels first described this in 1845:
‘When one individual inflicts bodily injury upon another such that death results, we call the deed manslaughter; when the assailant knew in advance that the injury would be fatal, we call his deed murder. But when society places hundreds of proletarians in such a position that they inevitably meet a too early and an unnatural death, one which is quite as much a death by violence as that by the sword or bullet; when it deprives thousands of the necessaries of life, places them under conditions in which they cannot live — forces them, through the strong arm of the law, to remain in such conditions until that death ensues which is the inevitable consequence — knows that these thousands of victims must perish, and yet permits these conditions to remain, its deed is murder just as surely as the deed of the single individual; disguised, malicious murder, murder against which none can defend himself, which does not seem what it is, because no man sees the murderer, because the death of the victim seems a natural one, since the offence is more one of omission than of commission. But murder it remains.’
The government didn’t send hitmen in with guns to massacre care home residents, but that doesn’t mean it isn’t a form of murder. Here’s how it happened.
Discharge and legislation
On the 27th of May, Boris Johnson – famed around the world for his honesty – declared ‘it’s just not true that there was some concerted effort to move people out of NHS beds into care homes.’ The NHS reserved 1800 beds in care homes right at the start of the pandemic and proceeded to discharge 25,000 patients between 17th March and 15th of April in England (plus about a thousand each in Wales and Scotland). Most weren’t even tested and, of those that were, patients who tested positive were discharged anyway (7 in Hull, 20 in Bristol and so on, 20% of care homes admitted patients with Covid-19 positive tests).
The government published guidance on 2nd April, titled ‘Admission and Care of Patients during Covid-19’, which stated:
‘the care sector also plays a vital role in accepting patients as they are discharged from hospital… Some of these patients may have Covid-19, whether symptomatic or asymptomatic… Hospitals around the country need as many beds as possible to support and treat an increasing number of Covid-19 cases. This means the NHS will seek to discharge more patients into care homes for the recovery period’.
No concerted effort, indeed. A Sky News survey of care homes found 70% of care homes felt pressured to take Covid-19 patients.
From April 15th, care homes received the formal ability to demand a test and reject Covid-19 patients, however, local councils replied by threatening to withhold pandemic funding unless they took patients in. Leading voices in the care sector also revealed that the £600m fund from the government actually prevented them spending the money on PPE for staff. Guidance was updated on September 16th reiterating that care homes should still be prepared to take Covid-19 positive patients from hospitals.
While the door was forced open to care homes, the door to hospitals was slammed shut. NHS hospitals were often operating a ‘no admissions’ policy for care home residents. The reason given for all of this was to prevent the NHS reaching capacity. Yet the Nightingale hospitals created specifically to deal with Covid-19 treated barely a trickle of patients, and then were largely kept ‘in hibernation’. The Nightingale hospital in London Docklands was arranged to have 4,000 beds, opening in early April, but the 7 hospitals across the entirety of England admitted hardly any patients at all (about 50 in London and approximately 100 in Manchester), and only briefly before they were put into ‘hibernation’ with potential capacity of several thousand beds and costing tens of millions in maintenance. Moreover, the NHS did not near capacity at any point; Alex Thomsen of Channel 4 news tweeted on 14th April: ‘Govt policy is to push recovering Covid hospital patients into care homes because NHS needs beds. Odd since no major hospital seems to be full and vast Nightingale field hospitals lie all but empty’.
Further to this, the fact that the government felt it necessary to grant legal immunity to health services and local authorities providing care for disabled people with the 2020 Coronavirus Act on 25th March and essentially suspend the legal duty to meet the needs of the disabled, could be considered a smoking gun. When discussing these facts with various people I tend to get the response: if this were true, there’d be a huge outcry. Well, let’s hear it from the government’s own ministers and MPs. Ros Altmann, former government minister, said care home residents ‘are being abandoned like lambs to the slaughter.’ She told Today:
‘They are left without protective equipment, they can’t find it, or testing even if they request it, it’s not always given to them. They haven’t got the staff they need … and they feel that the NHS has kind of left them in the lurch. GPs are not coming into the care homes in the way that they used to and some are finding if people need to be hospitalised either that tends to be very difficult or if people are sent to hospital they are sent back very quickly and there are no tests so they don’t know if these people are infecting others in their care homes.’
Tory MP Geoffrey Clifton-Brown characterised government approach to care homes as a ‘pretty reckless policy.’ Even Jeremy Hunt attacked his own government and a cross-party public accounts committee reported on 29th July that the Department of Health and Social Care (DHSC) had continued with the policy ‘even once it was clear there was an emerging problem’, and the chair (Meg Hillier MP), said ‘our care homes were effectively thrown to the wolves, and the virus has ravaged some of them.’
In response to criticism, Health Secretary Matt Hancock simply stated that it was not illegal. Boris Johnson shifted blame onto the care homes themselves: ‘We discovered too many care homes didn't really follow the procedures in the way that they could have.’ However, they followed the procedure of accepting Covid-19 positive patients as a fait-accompli – this is what caused the death toll. Labour provided zero opposition and their Five Point Plan in September didn’t even mention the seeding of the virus among those most vulnerable to it.
Floating cover staff, inspectors, and testing
The virus was further spread by allowing floating cover staff to move between different care homes, according to a study using genome tracking by Public Health England (PHE). Conducted from 11th to 13th April, results were known since – at the latest – the end of April, but weren’t circulated to care homes until weeks later. During this time at least 2,500 people died in English care homes. A report as far back as 2018 from flu pandemic planners warned ministers about controlling ‘cross-infection’ from such frontline temporary care workers.
A further document by PHE in 2019 regarding flu pandemic prep urged operators to avoid moving staff between homes and floors, yet the DHSC’s plan published on 16th April refrained from giving this same guidance which is so crucial in saving lives. In November The Telegraph reported that the government still hadn’t stopped agency workers from ‘roving’ across multiple sites, yet the spread of infection in care homes accounted for 82% of multiple outbreaks in the four weeks prior to the 8th of October, according to PHE.
In August the Care Quality Commission was repeatedly denied testing for its inspectors, a further risk of spread between 500 care homes planning to be inspected over a six-week period. The care sector trade union, GMB, predicted that inspectors would spread the virus ‘like wildfire’ through care homes: ‘we can’t comprehend why the government would deny inspectors access to testing.’ Technically, care staff have been eligible for tests since 28th April 2020, but the DHSC capped the daily amount of care home tests at 30,000 (both staff and residents). Tests were outright denied to people with learning disabilities and autism in care homes. Government guidance from the 15th April and updated on 14th May stated: 'you can only get tests if your care home looks after older people or people with dementia.' By the June 6th deadline for testing all care sector staff, the government had only managed about a third.
DNRs & frailty scale
At the beginning of the pandemic a ‘frailty index’ was created by the National Institute for Health and Care Excellence (NICE) to assess viability for critical care – those scoring above five on a scale of nine would be considered potentially disqualified from critical care. That included the ‘moderately frail’ – the patients who need help with complex tasks like financial management, transport, or heavy housework. NICE were soon forced to make U-turn on their advice for the NHS to deny disabled people treatment, but only after threats of legal action from disability groups. This index didn’t have a huge amount of time to do much damage, but is nevertheless another major indication of intent. The use of ‘Do not attempt resuscitation’ notices, on the other hand, functioned in a similar way, but were unable to be stopped in their tracks.
DNR notices waive the patient’s right to life. Typically these are signed by doctors in consultation with patients or failing that, their families, in situations where it’s in the best interests of the patient, in terms of minimising suffering, for them not to be resuscitated. One in ten care homes were told to place blanket DNRs on their residents or found that decision was taken by NHS staff without consultation with patients or their families, a report in August by Queen’s Nursing Institute found. Other patients were given DNRs as soon as they caught Covid-19. Some care homes delayed calling ambulances because of the DNRs. Residents 'felt pressured to agree to an advance Covid-19 care plan that stated they would stay at home without treatment if they contracted the virus.'
GPs across the country were writing to vulnerable patients advising them to fill out DNR forms in order to prioritise more able-bodied cases of Covid-19. One GP in Somerset recommended that autistic adults in care homes needed DNRs and another in Scarborough tried to apply it to an 11-year-old boy with cancer. Between July 2016 and December 2018, 19 hospital patients who died had ‘learning disabilities’ or ‘Down’s Syndrome’ given as the reason not to resuscitate. Turning Point, a learning disability care provider, stated that it had received an ‘unprecedented’ number of unlawful DNR orders for its patients. Hancock promised to ‘take action’ on wild use of DNRs, only after threat of a judicial review on 14th July. Yet, as late as October a press release by Amnesty International stated,
‘The horrifyingly widespread use of [Do not attempt cardiopulmonary resuscitation] orders for care home residents is one of the most deeply disturbing scandals of the pandemic. There’s no doubt that this was a violation of residents’ human rights and could have caused avoidable deaths… As we speak, countless do-not-resuscitate orders may remain in people’s files. Many of these people could fall ill in the coming months… It is also imperative that mechanisms are urgently put in place to ensure that there is full awareness across the health and social care sector that do-not-resuscitate orders must never be interpreted as meaning a person should not be transferred to hospital or receive other types of medical treatment.’
Furthermore it was found that around two thirds of people with underlying conditions (such as diabetes, high blood pressure, respiratory issues like asthma) were denied care during the pandemic.
It doesn’t matter to what extent this was premeditated and fully deliberate. Whether the government actively wanted to kill residents or simply didn’t consider them worthy of keeping alive is moot; the outcome is the same: social murder. A massacre, in fact. The government does have a motive, it had the means and it had the opportunity. They’ve tried to maintain plausible deniability, and this will be accepted by those who are in the habit of whitewashing Britain’s crimes and murderousness even in the face of overwhelming evidence. The crimes of Britain are legion and include, pointedly, use of germ warfare to commit mass murder and even genocide (using disease against Native Americans and First Nations in what is now the USA, Canada and Australia, and then between 1940-1979 tested biological weapons, including anthrax, on its own citizens in Britain, affecting the elderly in particular). The Conservative Party openly talked about the elderly and the disabled as posing a problem and a financial burden, before the government actively funnelled a lethal virus into care homes which house the very people most vulnerable to the disease. They deprived them of testing, protective equipment and other essential resources. They allowed floating cover staff and inspectors to exacerbate the spread, denied residents access to hospitals and forced DNRs on them. Case closed.
Pitchfork Cosmonaut writes on anti-imperialist current affairs, history, and pop culture, and you can find them on Twitter @pitchforkcosmo.
With special thanks to Prolekult, whose dedicated ongoing research of this issue has been fundamental to the writing of this piece. Make sure to watch their incredible documentary on this topic: Camps of Dependence.
https://www.ebb-magazine.com/essays/bri ... -home-cull
"There is great chaos under heaven; the situation is excellent."
Re: Socialist Demands for the COVID-19 Crisis
COVAX AND ASTRAZENECA: TOOLS FOR A HUMANITARIAN EXTORTION OPERATION
25 Mar 2021 , 1:14 pm .
A few days ago, some information media published the news of an alleged agreement between the government of Nicolás Maduro and the anti-Chavista group apparently led by Juan Guaidó to buy vaccines through the Covax mechanism, between 1 million 425 thousand 600 and 2 million 409 thousand 600 vaccine dose made by AstraZeneca / Oxford.
To gain access to this lot, which would only cover approximately 2% of the Venezuelan population, Venezuela would have to pay $ 18 million to the Revolving Fund of the Pan American Health Organization (PAHO), an institution recognized by Covax.
This mechanism, made up of the World Health Organization (WHO), the Alliance for Vaccines (Gavi) and the Coalition for Innovations in Preparedness for Epidemics (Cepi), is an international alliance that seeks to guarantee equitable vaccines to each participating country in 2021. Participating organizations have served as lobby groups through which Big Pharma grants a small batch of its vaccine production to more than 100 countries with financial difficulties.
It has been criticized that the Covax mechanism only has relationships with Western pharmaceutical companies, attracted by the market that ensures the pandemic in terms of health and scientific research. This despite the fact that Pfizer / BioNTech barely guarantees 2% of its production to the fund and foresees income from vaccine sales of just over 15 billion dollars.
Other vaccines that have been approved in the initiative are, in addition to the aforementioned AstraZeneca and Pfizer, those from Novavax, Janssen and Sanofi GSK. Sputnik V recently ran for the mechanism, good news that would break Big Pharma's vampire monopoly.
ASTRAZENECA DOES NOT
The multiple complaints made against the vaccine and the distribution of AstraZeneca in Europe kept the focus on the pharmaceutical company , which maintains a record of irregularities and fraud in the last two decades. For a few days the application of its vaccine was suspended in several countries of the European Union (EU) and other parts of the world, until political and media pressure reversed this decision.
The Venezuelan government did similarly, which announced that the British pharmaceutical vaccine would never be approved, and was reiterated by Executive Vice President Delcy Rodríguez. The risks seem much greater with the application of this vaccine over those already approved in the Bolivarian Republic: the Russian Sputnik V and the Cuban Sovereign 02 and Abdala.
While the version was running that there was an agreement to access the benefits of Covax, the Bolivarian Government never ruled on the issue. In fact, the decision not to opt for the use of the AstraZeneca vaccine and the complaint that the Venezuelan State has sent innumerable communications to representatives of financial entities where the assets of the Bolivarian Republic are blocked abroad, making it impossible to count with these resources due to the efforts made by the Guaidó clan for the effective operation of the blockade against the country.
Given the context in which Venezuela lives, the simplest logic takes precedence: the State has its extremely limited resources as a result of the blockade and the criminal looting of its accounts abroad, promoted by the most belligerent anti-Chavez and ingratiating with the US establishment. That is why the country cannot risk paying for vaccines whose effectiveness and side effects are in question in the eyes of public and scientific opinion worldwide.
The best thing is to look for other options, as has been done with the Russian, Cuban and even Chinese institutions.

Venezuela receives its first batch of Sputnik V vaccines (Photo: Reuters)
The intention of pressing for the use of the doses manufactured by AstraZeneca by the anti-Chavismo has the sign of humanitarian extortion, a new chapter of the "Guaidó project" that has political failure with a psychological operation involved.
ANOTHER HUMANITARIAN EXTORTION OPERATION
Days before PAHO's announcement about the Covax mechanism and the questioned AstraZeneca vaccine, Juan Guaidó and his court of criminals rolled the news of the alleged "agreement" to buy vaccines. They played an advanced position, taking into account that the Bolivarian Government had already decided not to have the doses of the British company.
From the beginning it was one more media operation with the aim of generating informative and, therefore, perceptive chaos around the issue of vaccines and the management of the health crisis resulting from the pandemic in Venezuela, in which they intersect bureaucratic, political and criminal statements and actions by the anti-Chavista promoters of the conflict.
As an information operation, it is predictable, and the humanitarian concept is held hostage to introduce it in a context in which there is an obvious international scandal over the uses, modes and products of AstraZeneca. Health as a commodity here takes an important profile to understand the cover-up of this important company of the global pharmaceutical capital.
In this way, the Covax mechanism is being used as a new instrument of confusion to attack Venezuela. The use in social networks of the hashtag #DejenEntrarLasVacunas is the tactical expression of this psychological operation, which combines the discourse of criminalization against the target ("the Chavista elite has already been vaccinated") and the imposition of a false narrative version in their denomination of origin. ("the regime does not want you to be vaccinated").
For international screens, it is understood that the Maduro government does not approve the use of the AstraZeneca product due to indolence and "social control" from a dictatorial position, when the decision is based on empirically scientific reasons. It is not a victimizing position. There is no ethical or moral reason, much less related to the current pandemic moment, for which a vaccine can be imposed on the country through media pressure that is being questioned by many other States in the world.
Venezuela has one of the best records of care and containment of the coronavirus. It has done so by creating its own large-scale registration system and house-to-house care for each suspected infected person, which includes popular mobilization, multidimensional methods to combat COVID and scientific innovation. It is an effective system that is being tested again with the Brazilian variant of protagonist in this second pandemic wave in the country.
Given the evidence recorded in its management of the pandemic, Venezuela is able to evaluate and decide which is the best vaccination strategy. It is a question of sovereignty and political firmness, a decision made by empirical and scientific rigors. Especially if it is related to a company whose record is as obscure as AstraZeneca.
https://misionverdad.com/venezuela/cova ... umanitaria
Google Translator
25 Mar 2021 , 1:14 pm .
A few days ago, some information media published the news of an alleged agreement between the government of Nicolás Maduro and the anti-Chavista group apparently led by Juan Guaidó to buy vaccines through the Covax mechanism, between 1 million 425 thousand 600 and 2 million 409 thousand 600 vaccine dose made by AstraZeneca / Oxford.
To gain access to this lot, which would only cover approximately 2% of the Venezuelan population, Venezuela would have to pay $ 18 million to the Revolving Fund of the Pan American Health Organization (PAHO), an institution recognized by Covax.
This mechanism, made up of the World Health Organization (WHO), the Alliance for Vaccines (Gavi) and the Coalition for Innovations in Preparedness for Epidemics (Cepi), is an international alliance that seeks to guarantee equitable vaccines to each participating country in 2021. Participating organizations have served as lobby groups through which Big Pharma grants a small batch of its vaccine production to more than 100 countries with financial difficulties.
It has been criticized that the Covax mechanism only has relationships with Western pharmaceutical companies, attracted by the market that ensures the pandemic in terms of health and scientific research. This despite the fact that Pfizer / BioNTech barely guarantees 2% of its production to the fund and foresees income from vaccine sales of just over 15 billion dollars.
Other vaccines that have been approved in the initiative are, in addition to the aforementioned AstraZeneca and Pfizer, those from Novavax, Janssen and Sanofi GSK. Sputnik V recently ran for the mechanism, good news that would break Big Pharma's vampire monopoly.
ASTRAZENECA DOES NOT
The multiple complaints made against the vaccine and the distribution of AstraZeneca in Europe kept the focus on the pharmaceutical company , which maintains a record of irregularities and fraud in the last two decades. For a few days the application of its vaccine was suspended in several countries of the European Union (EU) and other parts of the world, until political and media pressure reversed this decision.
The Venezuelan government did similarly, which announced that the British pharmaceutical vaccine would never be approved, and was reiterated by Executive Vice President Delcy Rodríguez. The risks seem much greater with the application of this vaccine over those already approved in the Bolivarian Republic: the Russian Sputnik V and the Cuban Sovereign 02 and Abdala.
While the version was running that there was an agreement to access the benefits of Covax, the Bolivarian Government never ruled on the issue. In fact, the decision not to opt for the use of the AstraZeneca vaccine and the complaint that the Venezuelan State has sent innumerable communications to representatives of financial entities where the assets of the Bolivarian Republic are blocked abroad, making it impossible to count with these resources due to the efforts made by the Guaidó clan for the effective operation of the blockade against the country.
Given the context in which Venezuela lives, the simplest logic takes precedence: the State has its extremely limited resources as a result of the blockade and the criminal looting of its accounts abroad, promoted by the most belligerent anti-Chavez and ingratiating with the US establishment. That is why the country cannot risk paying for vaccines whose effectiveness and side effects are in question in the eyes of public and scientific opinion worldwide.
The best thing is to look for other options, as has been done with the Russian, Cuban and even Chinese institutions.
Venezuela receives its first batch of Sputnik V vaccines (Photo: Reuters)
The intention of pressing for the use of the doses manufactured by AstraZeneca by the anti-Chavismo has the sign of humanitarian extortion, a new chapter of the "Guaidó project" that has political failure with a psychological operation involved.
ANOTHER HUMANITARIAN EXTORTION OPERATION
Days before PAHO's announcement about the Covax mechanism and the questioned AstraZeneca vaccine, Juan Guaidó and his court of criminals rolled the news of the alleged "agreement" to buy vaccines. They played an advanced position, taking into account that the Bolivarian Government had already decided not to have the doses of the British company.
From the beginning it was one more media operation with the aim of generating informative and, therefore, perceptive chaos around the issue of vaccines and the management of the health crisis resulting from the pandemic in Venezuela, in which they intersect bureaucratic, political and criminal statements and actions by the anti-Chavista promoters of the conflict.
As an information operation, it is predictable, and the humanitarian concept is held hostage to introduce it in a context in which there is an obvious international scandal over the uses, modes and products of AstraZeneca. Health as a commodity here takes an important profile to understand the cover-up of this important company of the global pharmaceutical capital.
In this way, the Covax mechanism is being used as a new instrument of confusion to attack Venezuela. The use in social networks of the hashtag #DejenEntrarLasVacunas is the tactical expression of this psychological operation, which combines the discourse of criminalization against the target ("the Chavista elite has already been vaccinated") and the imposition of a false narrative version in their denomination of origin. ("the regime does not want you to be vaccinated").
For international screens, it is understood that the Maduro government does not approve the use of the AstraZeneca product due to indolence and "social control" from a dictatorial position, when the decision is based on empirically scientific reasons. It is not a victimizing position. There is no ethical or moral reason, much less related to the current pandemic moment, for which a vaccine can be imposed on the country through media pressure that is being questioned by many other States in the world.
Venezuela has one of the best records of care and containment of the coronavirus. It has done so by creating its own large-scale registration system and house-to-house care for each suspected infected person, which includes popular mobilization, multidimensional methods to combat COVID and scientific innovation. It is an effective system that is being tested again with the Brazilian variant of protagonist in this second pandemic wave in the country.
Given the evidence recorded in its management of the pandemic, Venezuela is able to evaluate and decide which is the best vaccination strategy. It is a question of sovereignty and political firmness, a decision made by empirical and scientific rigors. Especially if it is related to a company whose record is as obscure as AstraZeneca.
https://misionverdad.com/venezuela/cova ... umanitaria
Google Translator
"There is great chaos under heaven; the situation is excellent."